

Patient-specific detection of cerebral blood flow alterations as assessed by arterial spin labeling in drug-resistant epileptic patients
- PMID: 25946055
- PMCID: PMC4422723
- DOI: 10.1371/journal.pone.0123975
Patient-specific detection of cerebral blood flow alterations as assessed by arterial spin labeling in drug-resistant epileptic patients
Abstract
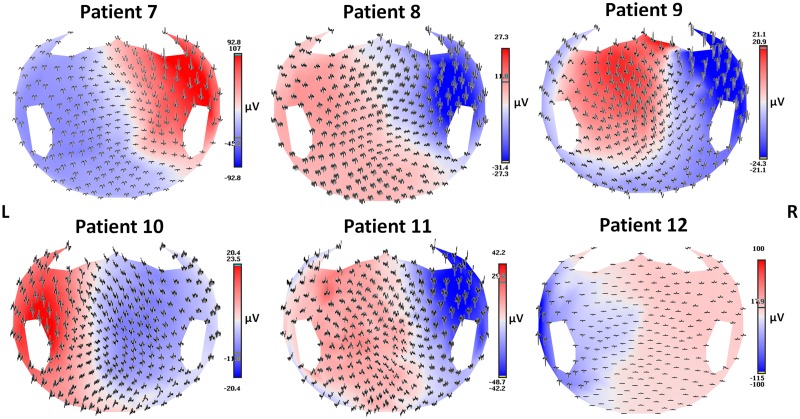
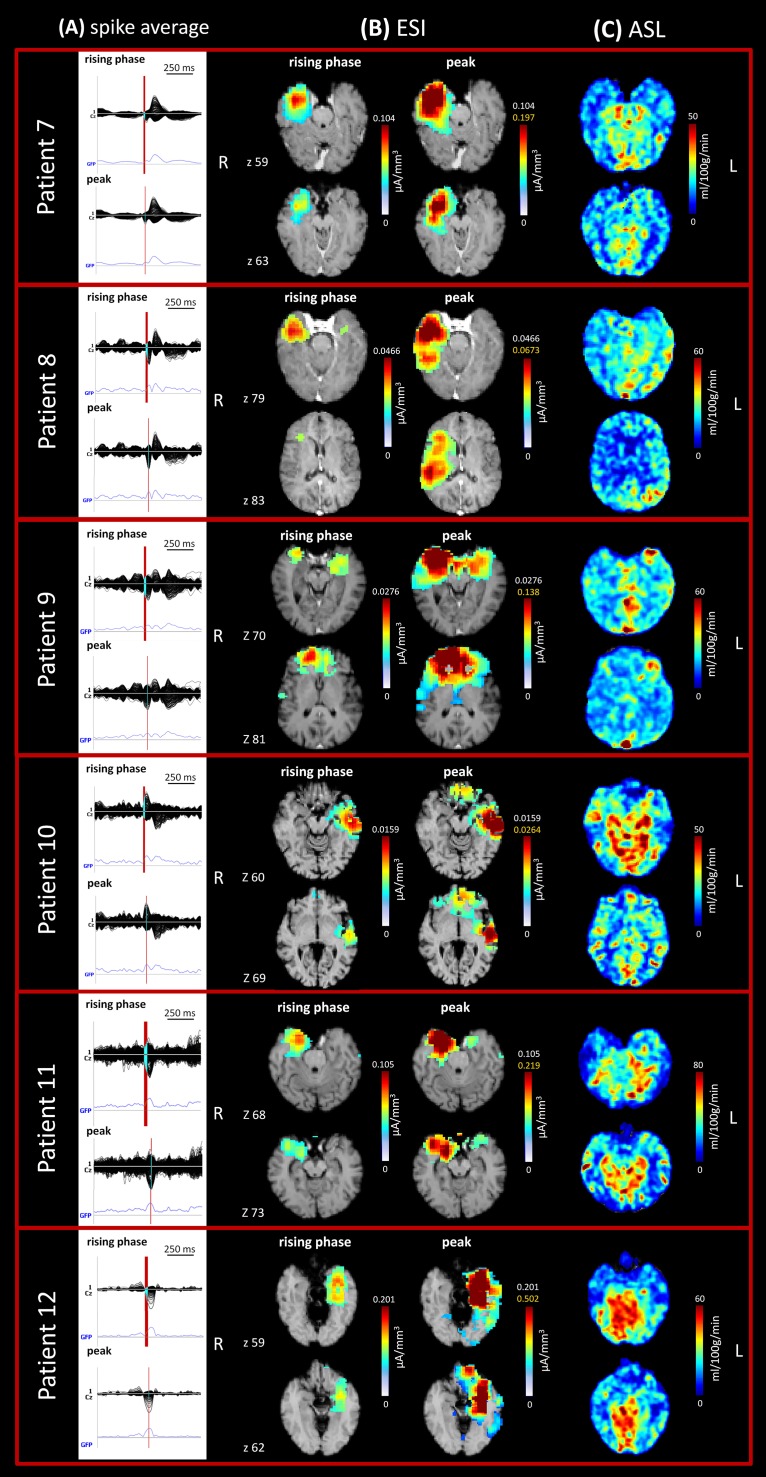
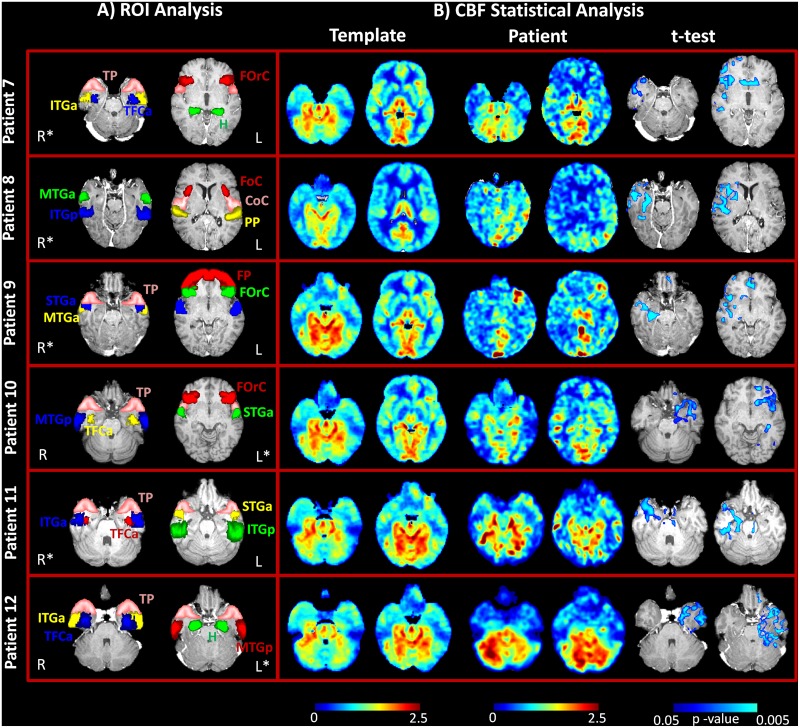
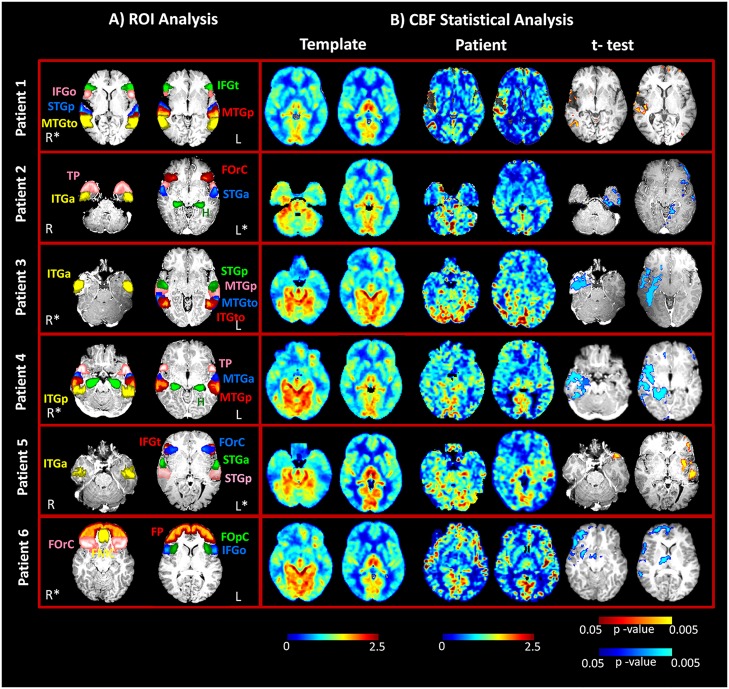
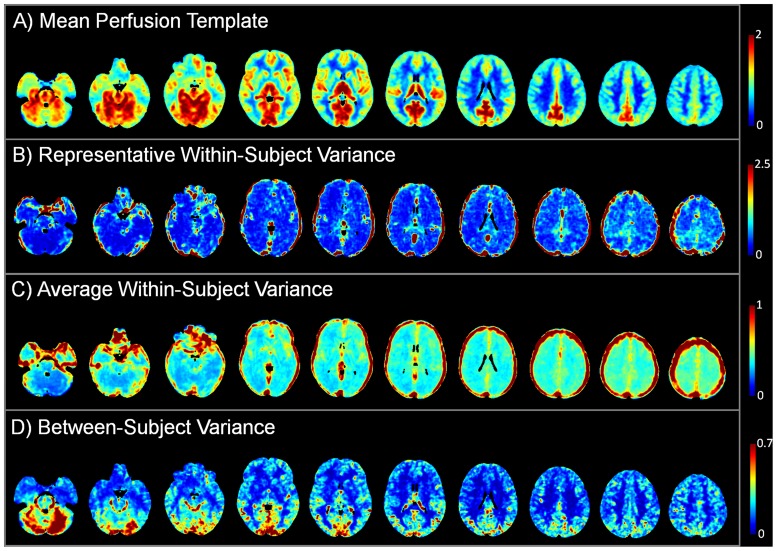
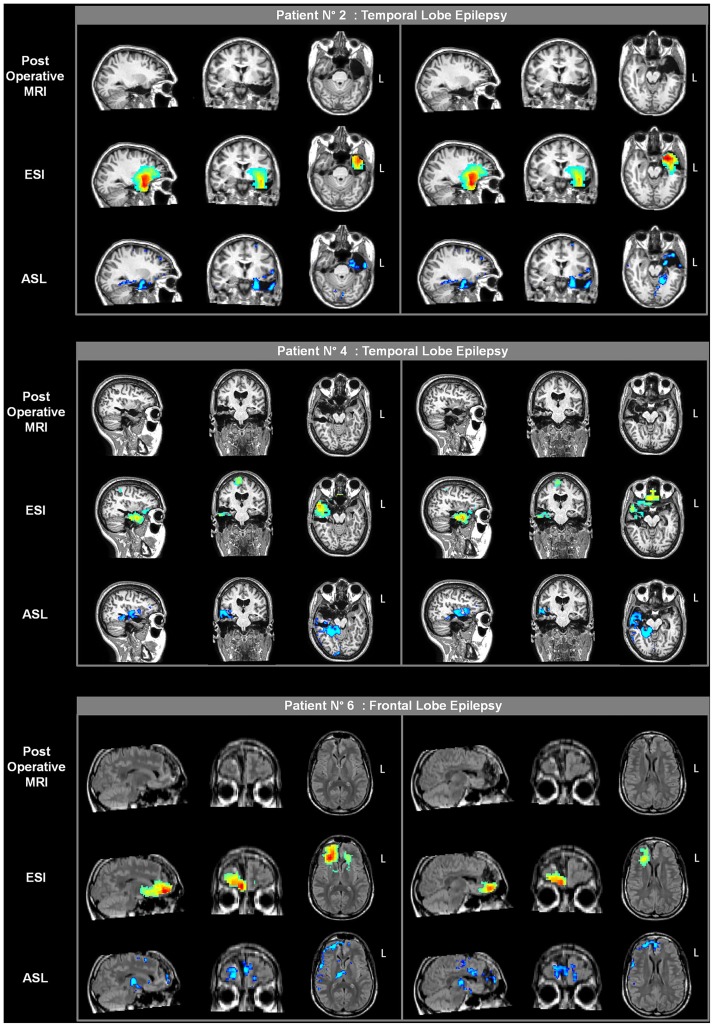
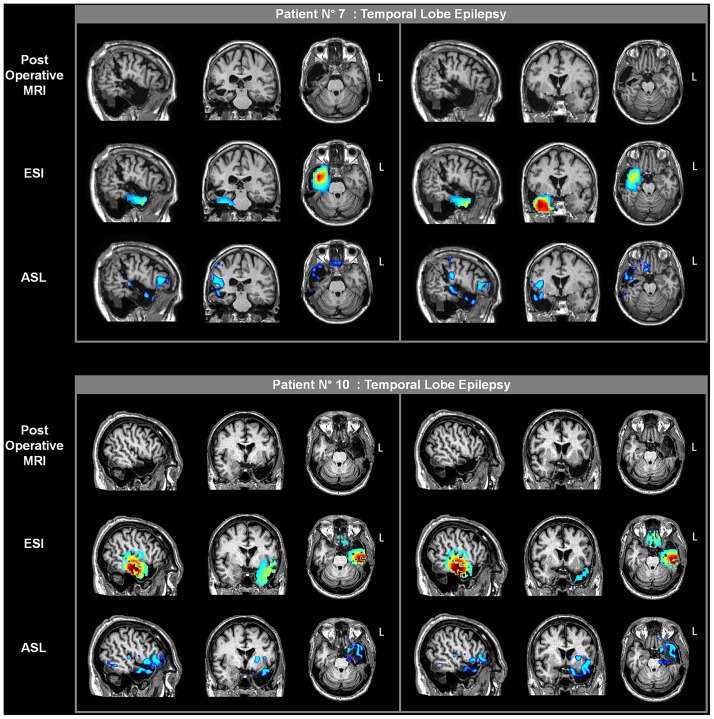
Electrophysiological and hemodynamic data can be integrated to accurately and precisely identify the generators of abnormal electrical activity in drug-resistant focal epilepsy. Arterial Spin Labeling (ASL), a magnetic resonance imaging (MRI) technique for quantitative noninvasive measurement of cerebral blood flow (CBF), can provide a direct measure of variations in cerebral perfusion associated with the epileptic focus. In this study, we aimed to confirm the ASL diagnostic value in the identification of the epileptogenic zone, as compared to electrical source imaging (ESI) results, and to apply a template-based approach to depict statistically significant CBF alterations. Standard video-electroencephalography (EEG), high-density EEG, and ASL were performed to identify clinical seizure semiology and noninvasively localize the epileptic focus in 12 drug-resistant focal epilepsy patients. The same ASL protocol was applied to a control group of 17 healthy volunteers from which a normal perfusion template was constructed using a mixed-effect approach. CBF maps of each patient were then statistically compared to the reference template to identify perfusion alterations. Significant hypo- and hyperperfused areas were identified in all cases, showing good agreement between ASL and ESI results. Interictal hypoperfusion was observed at the site of the seizure in 10/12 patients and early postictal hyperperfusion in 2/12. The epileptic focus was correctly identified within the surgical resection margins in the 5 patients who underwent lobectomy, all of which had good postsurgical outcomes. The combined use of ESI and ASL can aid in the noninvasive evaluation of drug-resistant epileptic patients.
Conflict of interest statement
Figures
References
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med. 2001; 345: 311–318. - PubMed
-
- Téllez-Zenteno JF, Dhar R, Wiebe S. Long-term seizure outcomes following epilepsy surgery: a systematic review and meta-analysis. Brain 2005; 128: 1188 –1198. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
