

Effect of performance improvement programs on compliance with sepsis bundles and mortality: a systematic review and meta-analysis of observational studies
- PMID: 25946168
- PMCID: PMC4422717
- DOI: 10.1371/journal.pone.0125827
Effect of performance improvement programs on compliance with sepsis bundles and mortality: a systematic review and meta-analysis of observational studies
Abstract
Background: Several reports suggest that implementation of the Surviving Sepsis Campaign (SSC) guidelines is associated with mortality reduction in sepsis. However, adherence to the guideline-based resuscitation and management sepsis bundles is still poor.
Objective: To perform a systematic review of studies evaluating the impact of performance improvement programs on compliance with Surviving Sepsis Campaign (SSC) guideline-based bundles and/or mortality.
Data sources: Medline (PubMed), Scopus and Intercollegiate Studies Institute Web of Knowledge databases from 2004 (first publication of the SSC guidelines) to October 2014.
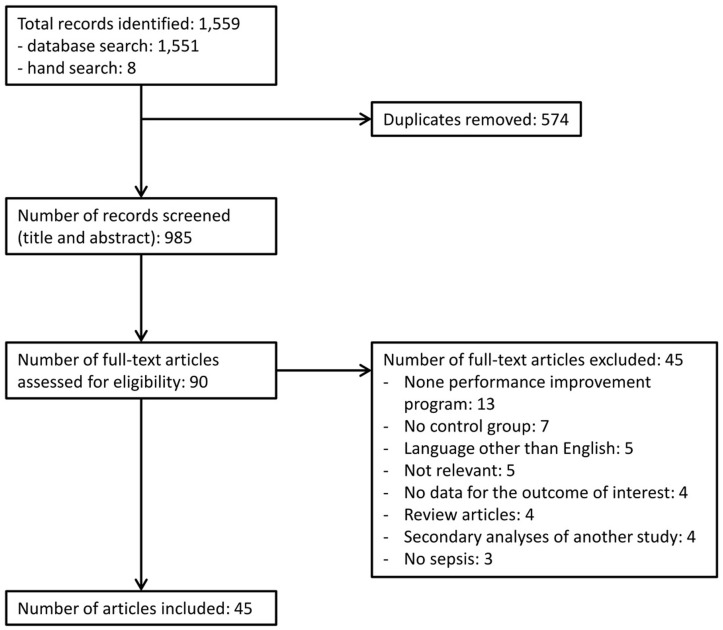
Study selection: Studies on adult patients with sepsis, severe sepsis or septic shock that evaluated changes in compliance to individual/combined bundle targets and/or mortality following the implementation of performance improvement programs. Interventions may consist of educational programs, process changes or both.
Data extraction: Data from the included studies were extracted independently by two authors. Unadjusted binary data were collected in order to calculate odds ratios (OR) for compliance to individual/combined bundle targets. Adjusted (if available) or unadjusted data of mortality were collected. Random-effects models were used for the data synthesis.
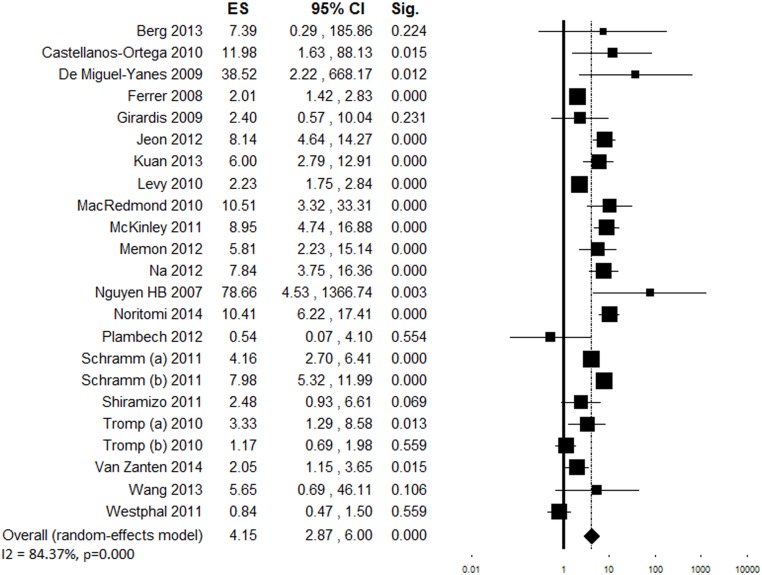
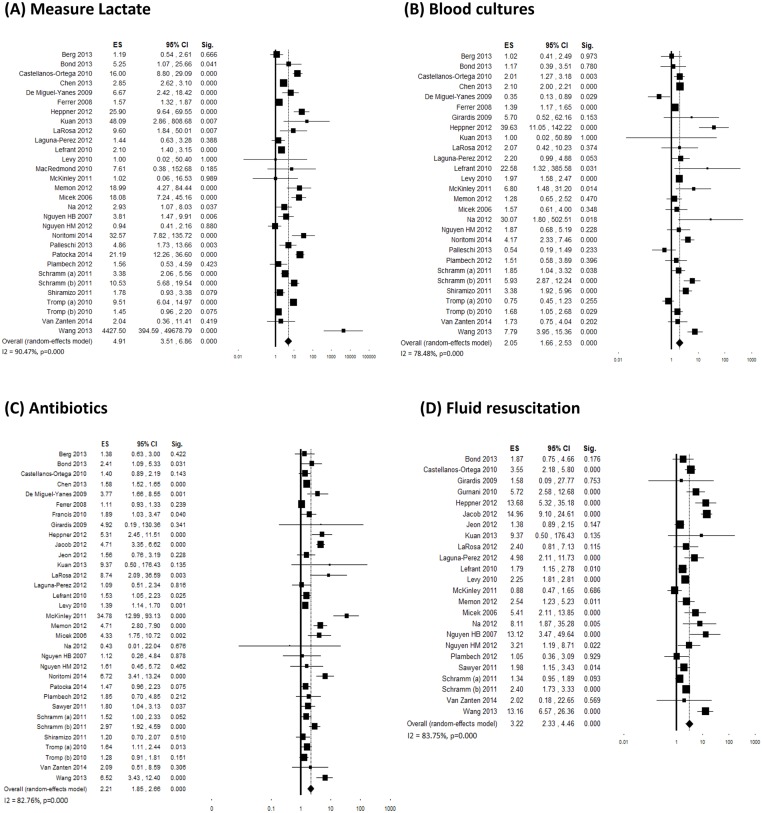
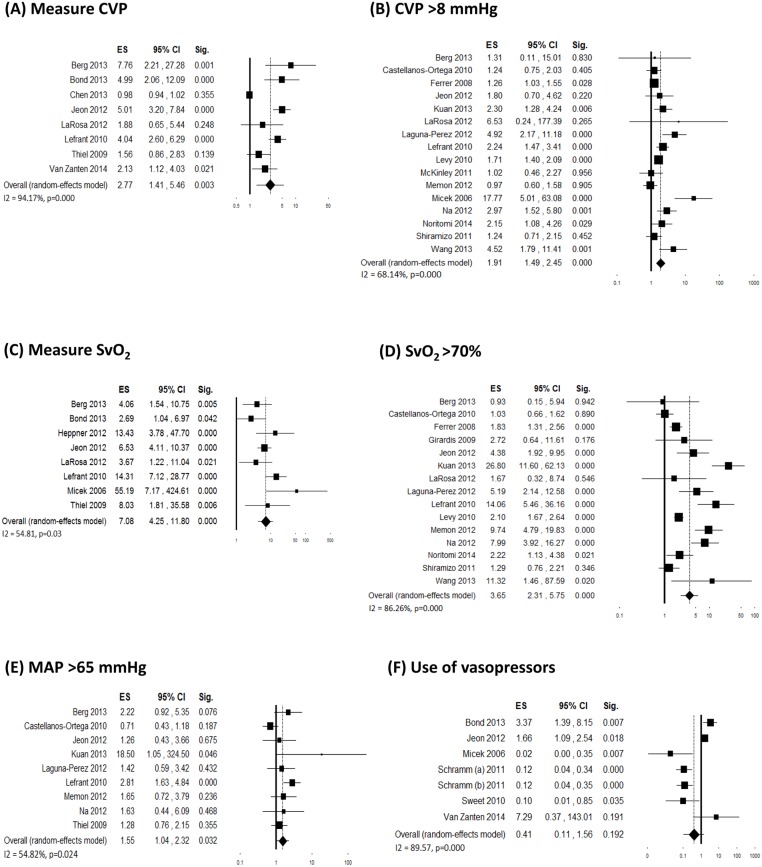
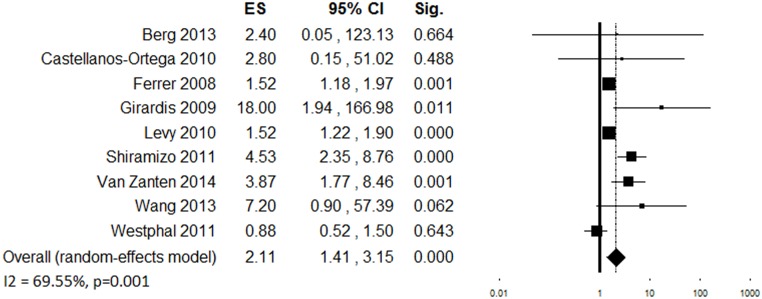
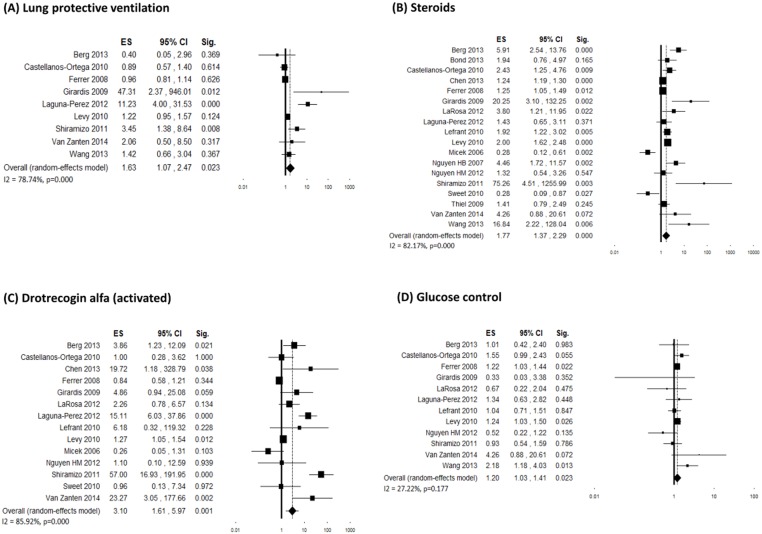
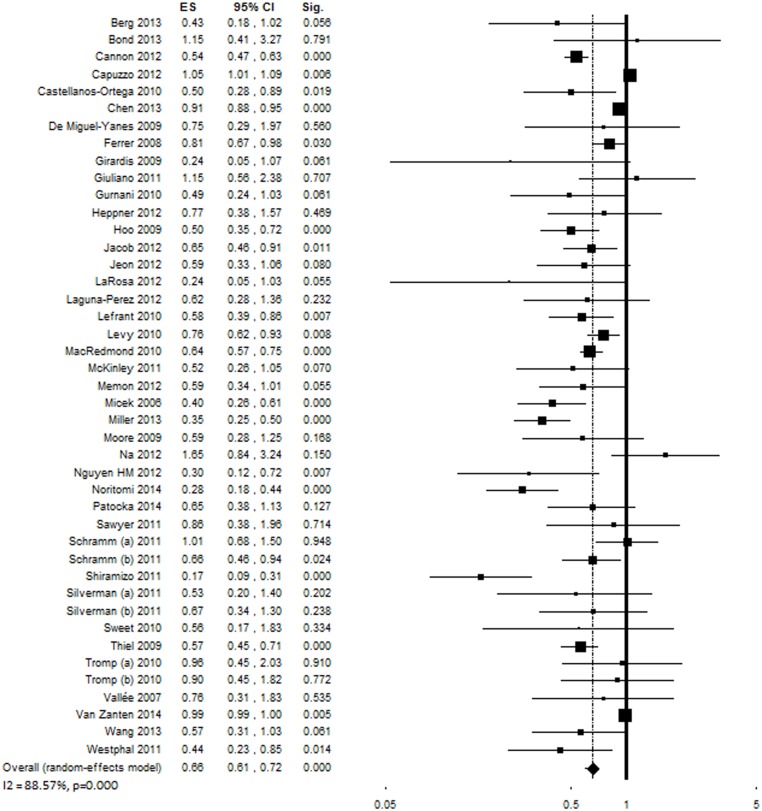
Results: Fifty observational studies were selected. Despite high inconsistency across studies, performance improvement programs were associated with increased compliance with the complete 6-hour bundle (OR = 4.12 [95% confidence interval 2.95-5.76], I(2) = 87.72%, k = 25, N = 50,081) and the complete 24-hour bundle (OR = 2.57 [1.74-3.77], I(2) = 85.22%, k = 11, N = 45,846) and with a reduction in mortality (OR = 0.66 [0.61-0.72], I(2) = 87.93%, k = 48, N = 434,447). Funnel plots showed asymmetry.
Conclusions: Performance improvement programs are associated with increased adherence to resuscitation and management sepsis bundles and with reduced mortality in patients with sepsis, severe sepsis or septic shock.
Conflict of interest statement
Figures
References
-
- Levy MM, Pronovost PJ, Dellinger RP, Townsend S, Resar RK, Clemmer TP, et al. Sepsis change bundles: Converting guidelines into meaningful change in behavior and clinical outcome. Crit Care Med. 2004; 32: S595–S597. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
