

Between-hospital variation in treatment and outcomes in extremely preterm infants
- PMID: 25946279
- PMCID: PMC4465092
- DOI: 10.1056/NEJMoa1410689
Between-hospital variation in treatment and outcomes in extremely preterm infants
Erratum in
-
Between-Hospital Variation in Treatment and Outcomes in Extremely Preterm Infants.N Engl J Med. 2015 Jun 18;372(25):2469. doi: 10.1056/NEJMx150023. N Engl J Med. 2015. PMID: 28282106 No abstract available.
Abstract
Background: Between-hospital variation in outcomes among extremely preterm infants is largely unexplained and may reflect differences in hospital practices regarding the initiation of active lifesaving treatment as compared with comfort care after birth.
Methods: We studied infants born between April 2006 and March 2011 at 24 hospitals included in the Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Data were collected for 4987 infants born before 27 weeks of gestation without congenital anomalies. Active treatment was defined as any potentially lifesaving intervention administered after birth. Survival and neurodevelopmental impairment at 18 to 22 months of corrected age were assessed in 4704 children (94.3%).
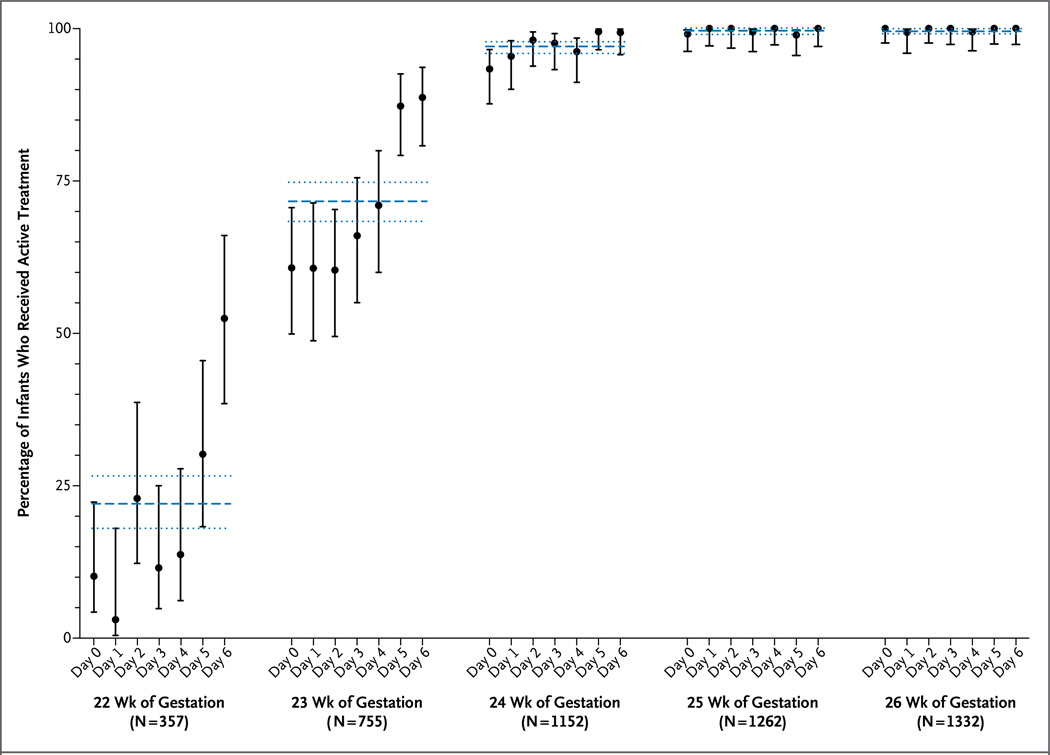
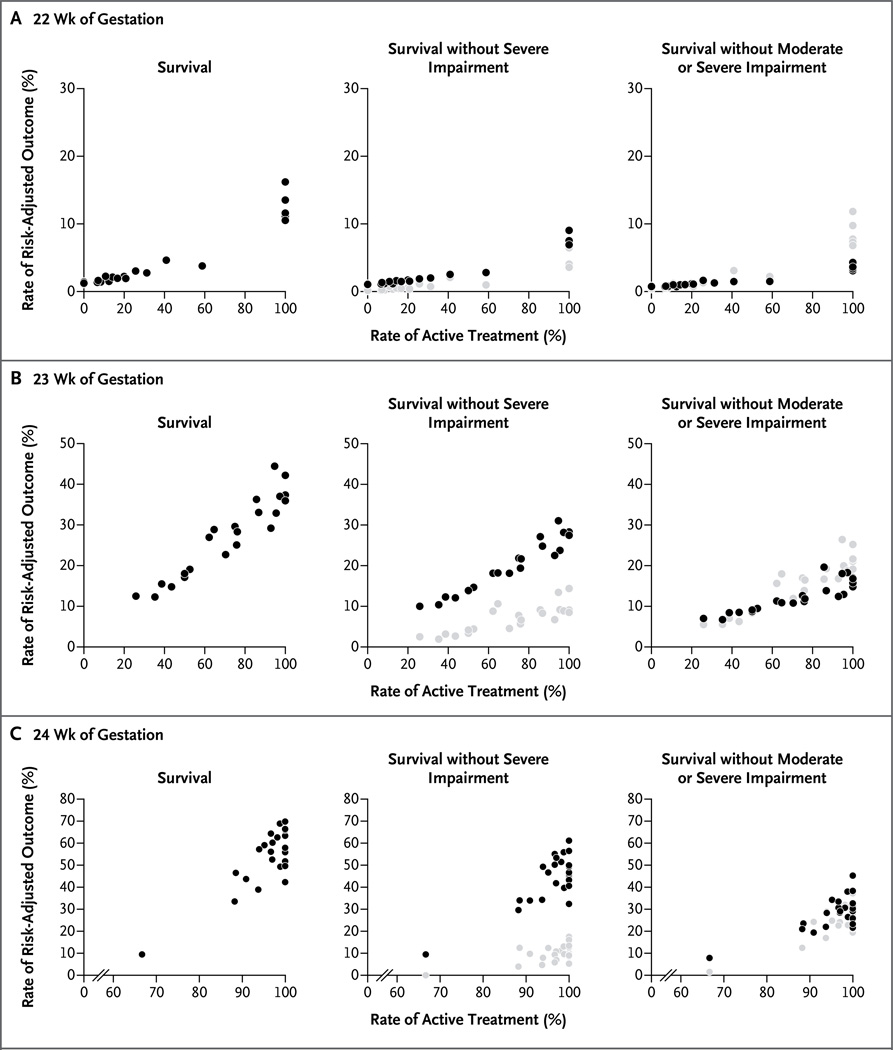
Results: Overall rates of active treatment ranged from 22.1% (interquartile range [IQR], 7.7 to 100) among infants born at 22 weeks of gestation to 99.8% (IQR, 100 to 100) among those born at 26 weeks of gestation. Overall rates of survival and survival without severe impairment ranged from 5.1% (IQR, 0 to 10.6) and 3.4% (IQR, 0 to 6.9), respectively, among children born at 22 weeks of gestation to 81.4% (IQR, 78.2 to 84.0) and 75.6% (IQR, 69.5 to 80.0), respectively, among those born at 26 weeks of gestation. Hospital rates of active treatment accounted for 78% and 75% of the between-hospital variation in survival and survival without severe impairment, respectively, among children born at 22 or 23 weeks of gestation, and accounted for 22% and 16%, respectively, among those born at 24 weeks of gestation, but the rates did not account for any of the variation in outcomes among those born at 25 or 26 weeks of gestation.
Conclusions: Differences in hospital practices regarding the initiation of active treatment in infants born at 22, 23, or 24 weeks of gestation explain some of the between-hospital variation in survival and survival without impairment among such patients. (Funded by the National Institutes of Health.).
Figures
Comment in
-
The elephant in the delivery room.N Engl J Med. 2015 May 7;372(19):1856-7. doi: 10.1056/NEJMe1502250. N Engl J Med. 2015. PMID: 25946286 No abstract available.
-
Hospital practice explains variation in outcomes in extremely premature infants, US study finds.BMJ. 2015 May 8;350:h2524. doi: 10.1136/bmj.h2524. BMJ. 2015. PMID: 25956663 No abstract available.
References
-
- Tyson JE, Younes N, Verter J, Wright LL. Viability, morbidity, and resource use among newborns of 501- to 800-g birth weight. JAMA. 1996;276:1645–1651. - PubMed
-
- Raju TNK, Mercer BM, Burchfield DJ, Joseph GF., Jr Periviable birth: executive summary of a joint workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists. Obstet Gynecol. 2014;123:1083–1096. - PubMed
-
- Bell EF. American Academy of Pediatrics Committee on Fetus and Newborn. Noninitiation or withdrawal of intensive care for high-risk newborns. Pediatrics. 2007;119:401–403. - PubMed
-
- Batton DG. Clinical report — antenatal counseling regarding resuscitation at an extremely low gestational age. Pediatrics. 2009;124:422–427. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD053124/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- UG1 HD087229/HD/NICHD NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- U10 HD027871/HD/NICHD NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- U10 HD053119/HD/NICHD NIH HHS/United States
- U01 HD036790/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD112093/HD/NICHD NIH HHS/United States
- U10 HD053109/HD/NICHD NIH HHS/United States
- U10 HD040689/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- UG1 HD021385/HD/NICHD NIH HHS/United States
- UG1 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- T32 GM007337/GM/NIGMS NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
- U10 HD053089/HD/NICHD NIH HHS/United States
- UL1 TR000371/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous