

High temporal resolution dynamic MRI and arterial input function for assessment of GFR in pediatric subjects
- PMID: 25946307
- PMCID: PMC4636486
- DOI: 10.1002/mrm.25731
High temporal resolution dynamic MRI and arterial input function for assessment of GFR in pediatric subjects
Abstract
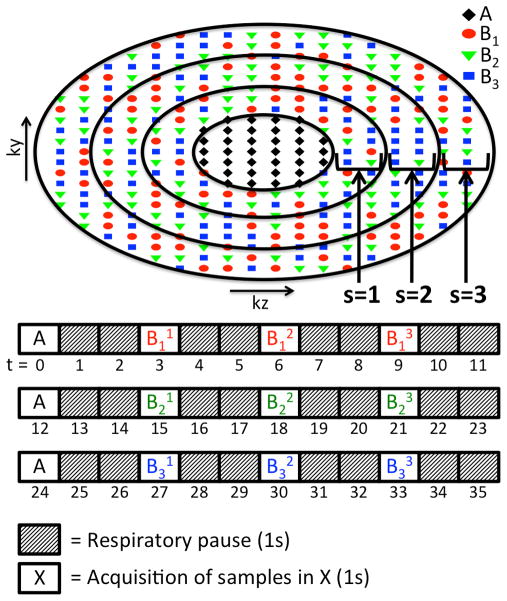
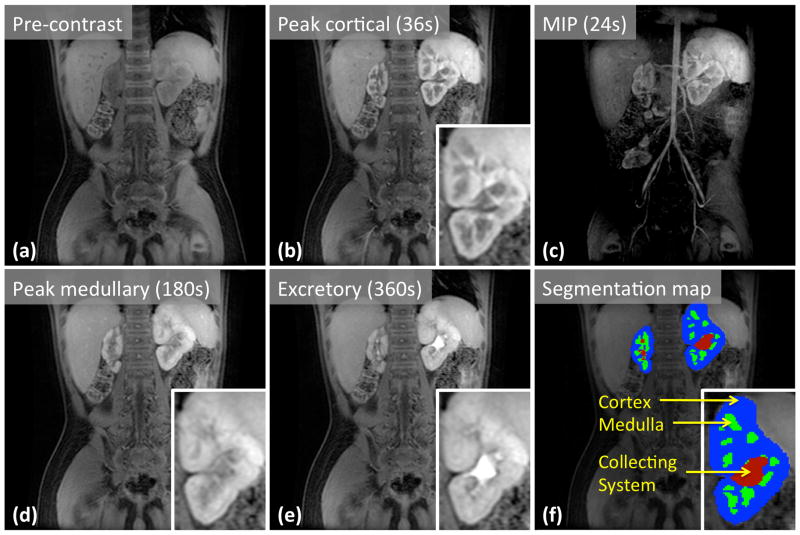
Purpose: To introduce a respiratory-gated high-spatiotemporal-resolution dynamic-contrast-enhanced MRI technique and a high-temporal-resolution aortic input function (HTR-AIF) estimation method for glomerular filtration rate (GFR) assessment in children.
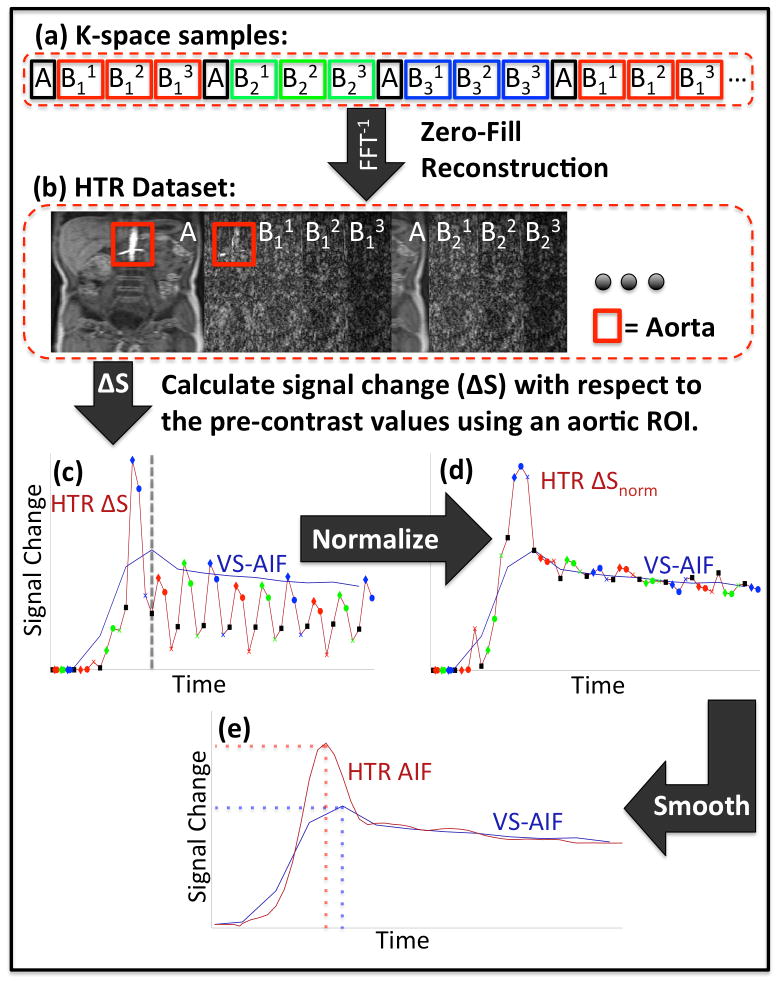
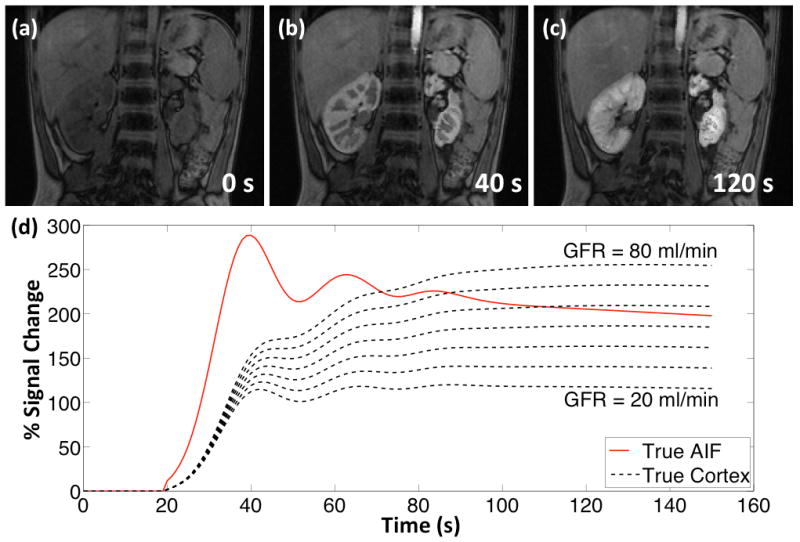
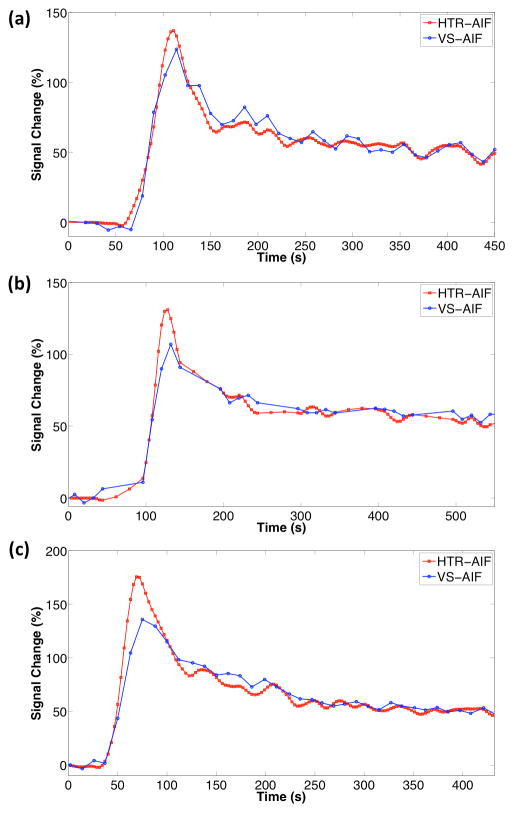
Methods: A high-spatiotemporal-resolution DCE-MRI method with view-shared reconstruction was modified to incorporate respiratory gating, and an AIF estimation method that uses a fraction of the k-space data from each respiratory period was developed (HTR-AIF). The method was validated using realistic digital phantom simulations and demonstrated on clinical subjects. The GFR estimates using HTR-AIF were compared with estimates obtained by using an AIF derived directly from the view-shared images.
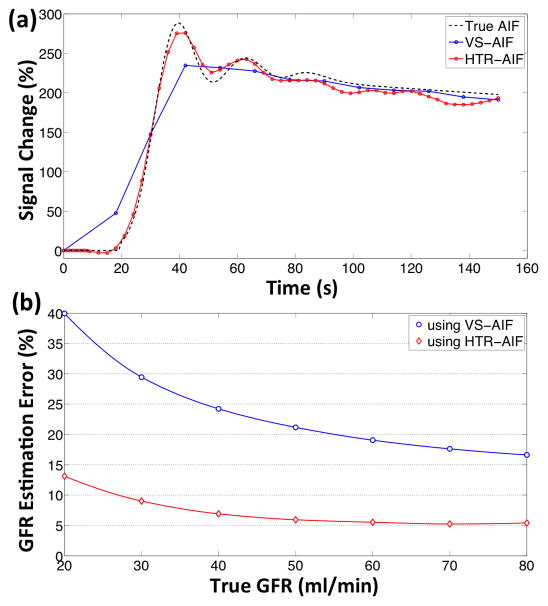
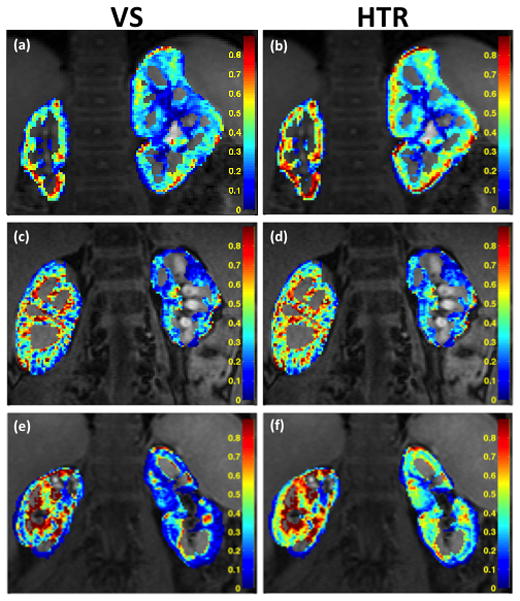
Results: Digital phantom simulations showed that using the HTR-AIF technique gives more accurate AIF estimates (RMSE = 0.0932) compared with the existing estimation method (RMSE = 0.2059) that used view-sharing (VS). For simulated GFR > 27 mL/min, GFR estimation error was between 32% and 17% using view-shared AIF, whereas estimation error was less than 10% using HTR-AIF. In all clinical subjects, the HTR-AIF method resulted in higher GFR estimations than the view-shared method.
Conclusion: The HTR-AIF method improves the accuracy of both the AIF and GFR estimates derived from the respiratory-gated acquisitions, and makes GFR estimation feasible in free-breathing pediatric subjects.
Keywords: arterial input function estimation; dynamic contrast enhancement; glomerular filtration rate estimation; high spatiotemporal resolution dynamic imaging; urography.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Sigmund G, Stoever B, Zimmerhackl LB, Frankenschmidt A, Nitzsche E, Leititis JU, Struwe FE, Hennig J. RARE-MR-urography in the diagnosis of upper urinary tract abnormalities in children. Pediatric radiology. 1991;21(6):416–420. - PubMed
-
- Regan F, Bohlman ME, Khazan R, Rodriguez R, Schultze-Haakh H. MR urography using HASTE imaging in the assessment of ureteric obstruction. AJR American journal of roentgenology. 1996;167(5):1115–1120. - PubMed
-
- Aerts P, Van Hoe L, Bosmans H, Oyen R, Marchal G, Baert AL. Breath-hold MR urography using the HASTE technique. AJR American journal of roentgenology. 1996;166(3):543–545. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
