

Analgesia and respiratory function after laparoscopic cholecystectomy in patients receiving ultrasound-guided bilateral oblique subcostal transversus abdominis plane block: a randomized double-blind study
- PMID: 25948166
- PMCID: PMC4434982
- DOI: 10.12659/MSM.893593
Analgesia and respiratory function after laparoscopic cholecystectomy in patients receiving ultrasound-guided bilateral oblique subcostal transversus abdominis plane block: a randomized double-blind study
Abstract
Background: Transversus abdominis plane (TAP) block has been shown to ameliorate postoperative pain after abdominal surgery. Postoperative pain-associated respiratory compromise has been the subject of several studies. Herein, we evaluate the effect of oblique subcostal TAP (OSTAP) block on postoperative pain and respiratory functions during the first 24 postoperative hours.
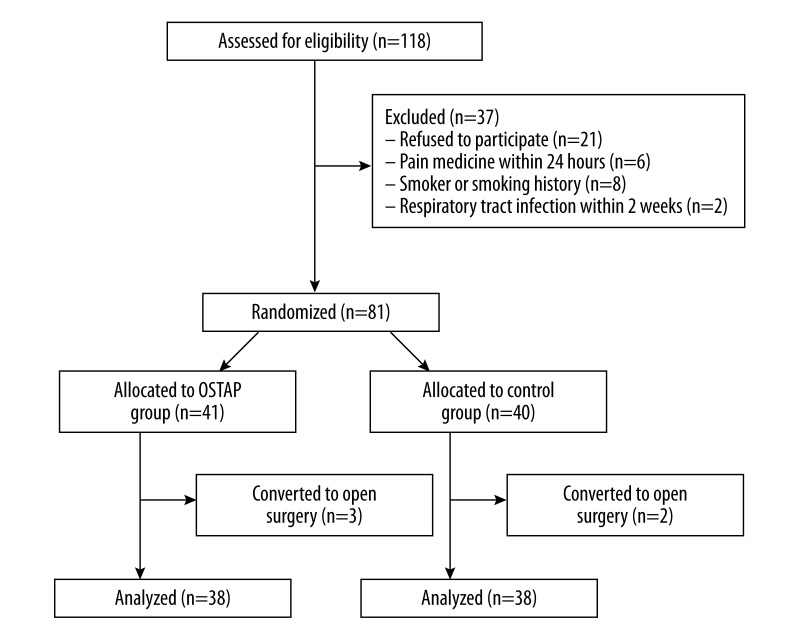
Material/methods: In this double-blind, randomized study, 76 patients undergoing laparoscopic cholecystectomy were assigned to either the OSTAP group (n=38) or control group (n=38). Bilateral ultrasound-guided OSTAP blocks were performed with 20 ml 0.25% bupivacaine after induction of general anesthesia. Both the OSTAP and control groups were treated with paracetamol, tenoxicam, and tramadol as required for postoperative analgesia. Visual Analog Scale (VAS) pain scores (while moving and at rest), forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), peak expiratory flow rate (PEFR), arterial blood gas variables, and opioid consumption were assessed during first 24 h.
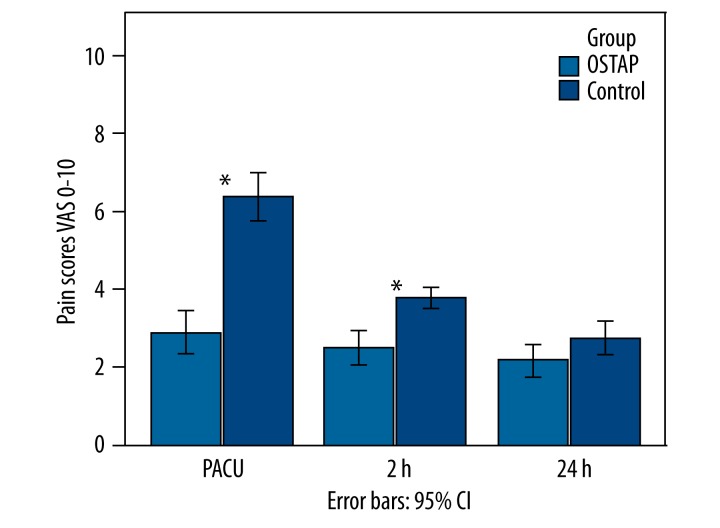
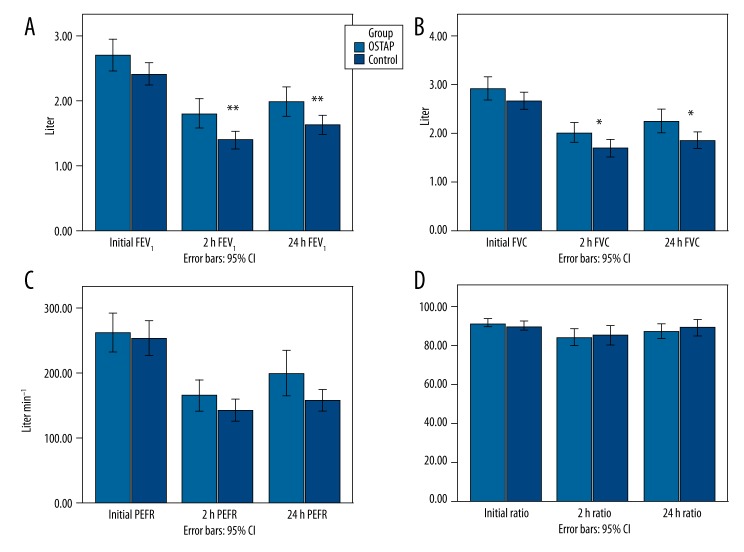
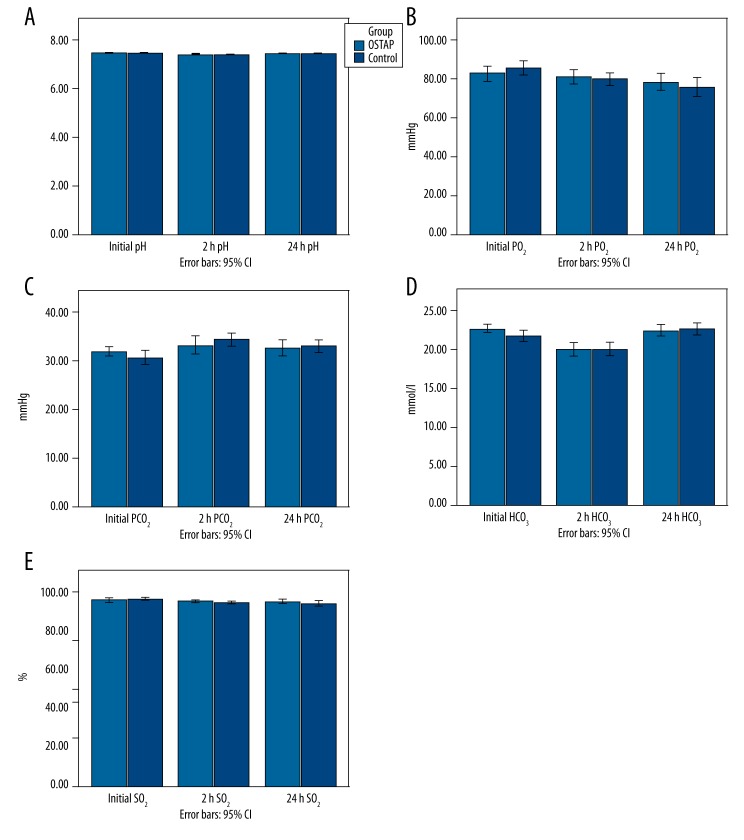
Results: VAS pain scores at rest and while moving were significantly lower in the OSTAP group on arrival to PACU and at 2 h postoperatively. The total postoperative tramadol requirement was significantly reduced at 0-2 h and 2-24 h in the OSTAP group. Postoperative deterioration in FEV1 and FVC was significantly less in the OSTAP group when compared to the control group (P<0.01 and P<0.05, respectively). There were no between-group differences in arterial blood gas variables.
Conclusions: After laparoscopic cholecystectomy, OSTAP block can provide significant improvement in respiratory function and better pain relief with lower opioid requirement.
Figures

References
-
- Slinger P. From the Journal archives: Postoperative analgesia: effect on lung volumes. Can J Anaesth. 2014;61(2):200–2. - PubMed
-
- Ali J, Weisel RD, Layug AB, et al. Consequences of postoperative alterations in respiratory mechanics. Am J Surg. 1974;128(3):376–82. - PubMed
-
- Brull R, McCartney CJ, Chan VW, et al. Neurological complications after regional anesthesia: contemporary estimates of risk. Anesth Analg. 2007;104(4):965–74. - PubMed
-
- Rigg JR, Jamrozik K, Myles PS, et al. Epidural anaesthesia and analgesia and outcome of major surgery: a randomised trial. Lancet. 2002;359(9314):1276–82. - PubMed
-
- Staehr-Rye AK, Rasmussen LS, Rosenberg J, et al. Minimal impairment in pulmonary function following laparoscopic surgery. Acta Anaesthesiol Scand. 2014;58(2):198–205. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
