

The prevention, detection and management of cancer treatment-induced cardiotoxicity: a meta-review
- PMID: 25948399
- PMCID: PMC4427936
- DOI: 10.1186/s12885-015-1407-6
The prevention, detection and management of cancer treatment-induced cardiotoxicity: a meta-review
Abstract
Background: The benefits associated with some cancer treatments do not come without risk. A serious side effect of some common cancer treatments is cardiotoxicity. Increased recognition of the public health implications of cancer treatment-induced cardiotoxicity has resulted in a proliferation of systematic reviews in this field to guide practice. Quality appraisal of these reviews is likely to limit the influence of biased conclusions from systematic reviews that have used poor methodology related to clinical decision-making. The aim of this meta-review is to appraise and synthesise evidence from only high quality systematic reviews focused on the prevention, detection or management of cancer treatment-induced cardiotoxicity.
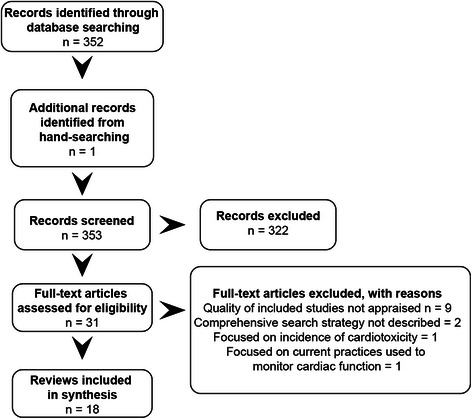
Methods: Using Cochrane methodology, we searched databases, citations and hand-searched bibliographies. Two reviewers independently appraised reviews and extracted findings. A total of 18 high quality systematic reviews were subsequently analysed, 67 % (n = 12) of these comprised meta-analyses.
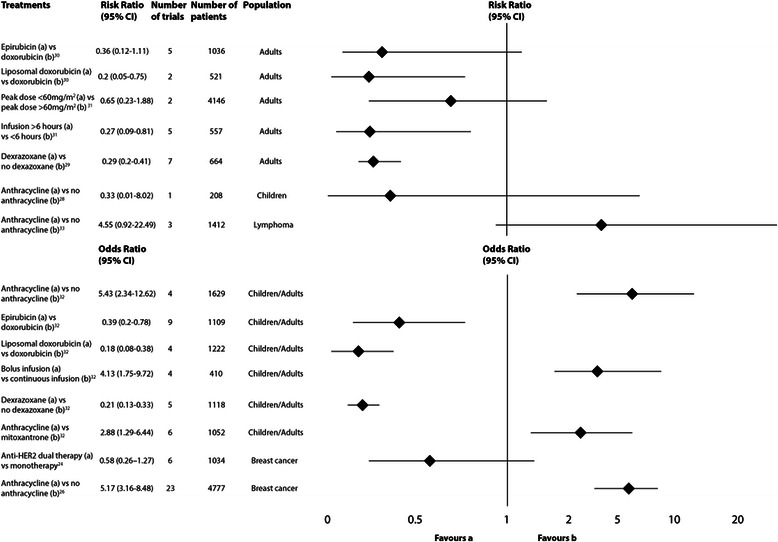
Results: One systematic review concluded that there is insufficient evidence regarding the utility of cardiac biomarkers for the detection of cardiotoxicity. The following strategies might reduce the risk of cardiotoxicity: 1) The concomitant administration of dexrazoxane with anthracylines; 2) The avoidance of anthracyclines where possible; 3) The continuous administration of anthracyclines (>6 h) rather than bolus dosing; and 4) The administration of anthracycline derivatives such as epirubicin or liposomal-encapsulated doxorubicin instead of doxorubicin. In terms of management, one review focused on medical interventions for treating anthracycline-induced cardiotoxicity during or after treatment of childhood cancer. Neither intervention (enalapril and phosphocreatine) was associated with statistically significant improvement in ejection fraction or mortality.
Conclusion: This review highlights the lack of high level evidence to guide clinical decision-making with respect to the detection and management of cancer treatment-associated cardiotoxicity. There is more evidence with respect to the prevention of this adverse effect of cancer treatment. This evidence, however, only applies to anthracycline-based chemotherapy in a predominantly adult population. There is no high-level evidence to guide clinical decision-making regarding the prevention, detection or management of radiation-induced cardiotoxicity.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
