

Misdiagnosis of Myocardial Infarction Related to Limitations of the Current Regulatory Approach to Define Clinical Decision Values for Cardiac Troponin
- PMID: 25948541
- PMCID: PMC4456170
- DOI: 10.1161/CIRCULATIONAHA.114.014129
Misdiagnosis of Myocardial Infarction Related to Limitations of the Current Regulatory Approach to Define Clinical Decision Values for Cardiac Troponin
Abstract
Background: Misdiagnosis of acute myocardial infarction (AMI) may significantly harm patients and may result from inappropriate clinical decision values (CDVs) for cardiac troponin (cTn) owing to limitations in the current regulatory process.
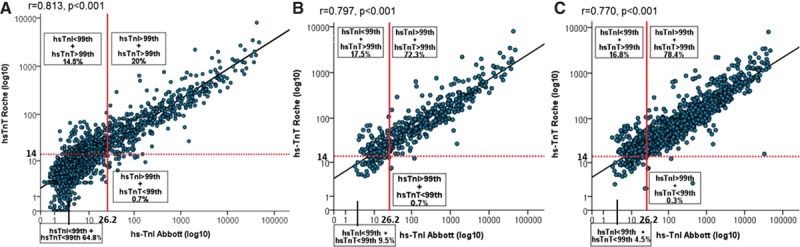
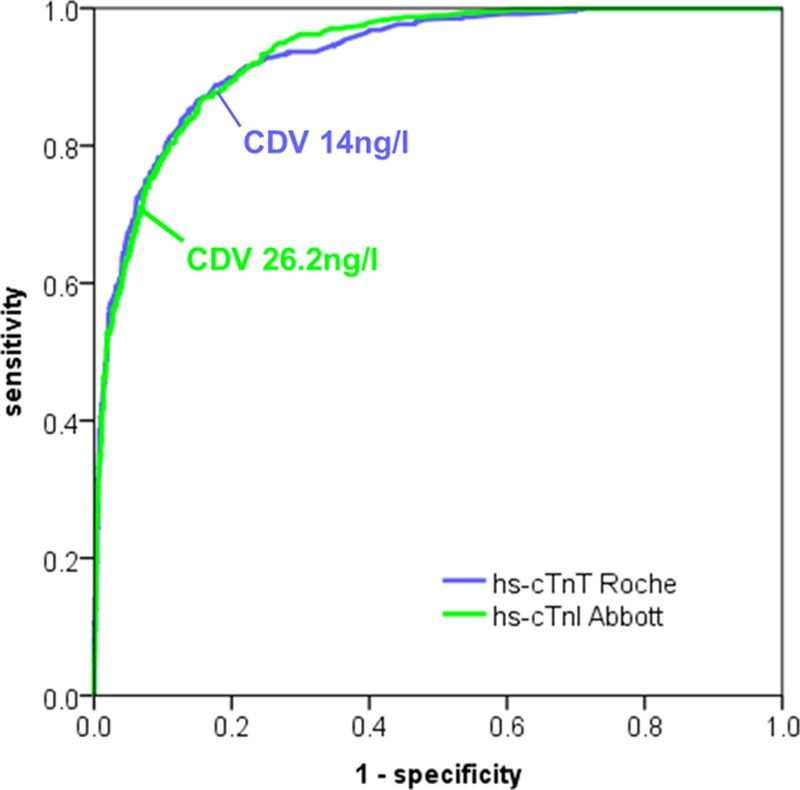
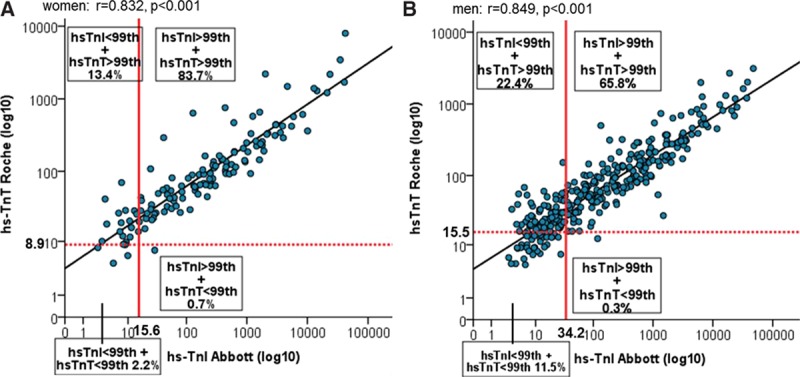
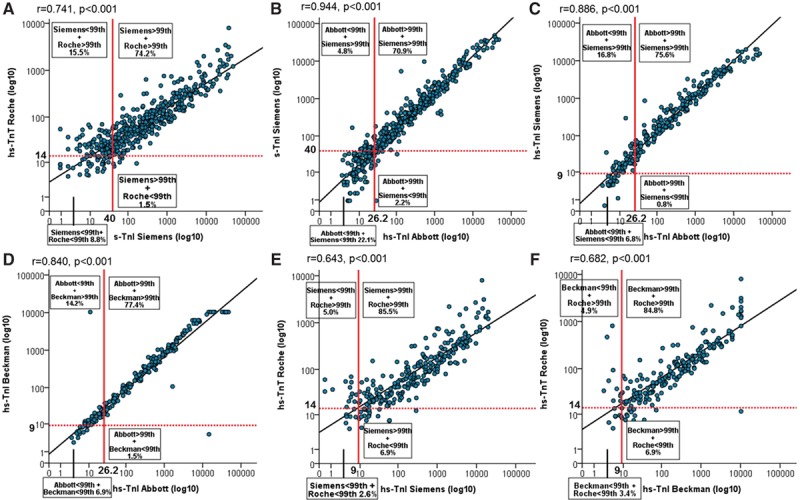
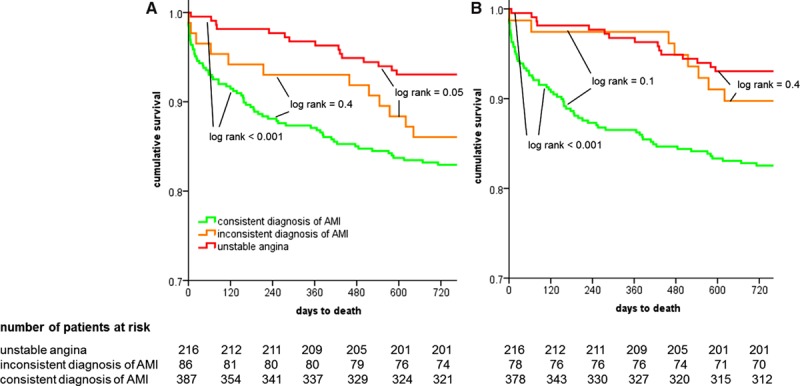
Methods and results: In an international, prospective, multicenter study, we quantified the incidence of inconsistencies in the diagnosis of AMI using fully characterized and clinically available high-sensitivity (hs) cTn assays (hs-cTnI, Abbott; hs-cTnT, Roche) among 2300 consecutive patients with suspected AMI. We hypothesized that the approved CDVs for the 2 assays are not biologically equivalent and might therefore contribute to inconsistencies in the diagnosis of AMI. Findings were validated by use of sex-specific CDVs and parallel measurements of other hs-cTnI assays. AMI was the adjudicated diagnosis in 473 patients (21%). Among these, 86 patients (18.2%) had inconsistent diagnoses when the approved uniform CDV was used. When sex-specific CDVs were used, 14.1% of female and 22.7% of male AMI patients had inconsistent diagnoses. Using biologically equivalent CDV reduced inconsistencies to 10% (P<0.001). These findings were confirmed with parallel measurements of other hs-cTn assays. The incidence of inconsistencies was only 7.0% for assays with CDVs that were nearly biologically equivalent. Patients with inconsistent AMI had long-term mortality comparable to that of patients with consistent diagnoses (P=NS) and a trend toward higher long-term mortality than patients diagnosed with unstable angina (P=0.05).
Conclusions: Currently approved CDVs are not biologically equivalent and contribute to major inconsistencies in the diagnosis of AMI. One of 5 AMI patients will receive a diagnosis other than AMI if managed with the alternative hs-cTn assay.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00470587.
Keywords: acute cardiac care; biological markers; myocardial infarction; troponin.
© 2015 The Authors.
Figures
Comment in
-
Is the 99th Percentile the Optimal Reference Limit to Diagnose Myocardial Infarction With High-Sensitivity Cardiac Troponin Assays in Patients With Chronic Kidney Disease?Circulation. 2015 Jun 9;131(23):2029-31. doi: 10.1161/CIRCULATIONAHA.115.016848. Epub 2015 May 6. Circulation. 2015. PMID: 25948540 No abstract available.
References
-
- Nawar EW, Niska RW, Xu J. National Hospital Ambulatory Medical Care Survey: 2005 emergency department summary. Adv Data. 2007;29:1–32. - PubMed
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE, Jr, Chavey WE 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non–ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e663–e828. - PubMed
-
- Hamm CW, Bassand JP, Agewall S, Bax JJ, Boersma E, Bueno H, Caso P, Dudek D, Gielen S, Huber K, Ohman M, Petrie MC, Sonntag F, Uva MS, Storey RF, Wijns W, Zahger D, ESC Committee for Practice Guidelines, Auricchio A, Baumgartner H, Ceconi C, Dean V, Deaton C, Fagard R, Funck-Brentano C, Hasdai D, Hoes A, Knuuti J, Kolh P, McDonagh T, Moulin C, Poldermans D, Popescu BA, Reiner Z, Sechtem U, Sirnes PA, Torbicki A, Vahanian A, Windecker S, Document R, Achenbach S, Badimon L, Bertrand M, Botker HE, Collet JP, Crea F, Danchin N, Falk E, Goudevenos J, Gulba D, Hambrecht R, Herrmann J, Kastrati A, Kjeldsen K, Kristensen SD, Lancellotti P, Mehilli J, Merkely B, Montalescot G, Neumann FJ, Neyses L, Perk J, Roffi M, Romeo F, Ruda M, Swahn E, Valgimigli M, Vrints CJ, Widimsky P. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation. Eur Hear J. 2011;32:2999–3054. - PubMed
-
- Brown TW, McCarthy ML, Kelen GD, Levy F. An epidemiologic study of closed emergency department malpractice claims in a national database of physician malpractice insurers. Acad Emerg Med. 2010;17:553–560. doi: 10.1111/j.1553-2712.2010.00729.x. - PubMed
-
- McCabe JM, Armstrong EJ, Kulkarni A, Hoffmayer KS, Bhave PD, Garg S, Patel A, MacGregor JS, Hsue P, Stein JC, Kinlay S, Ganz P. Prevalence and factors associated with false-positive ST-segment elevation myocardial infarction diagnoses at primary percutaneous coronary intervention–capable centers: a report from the Activate-SF registry. Arch Intern Med. 2012;172:864–871. doi: 10.1001/archinternmed.2012.945. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
