

Time from convulsive status epilepticus onset to anticonvulsant administration in children
- PMID: 25948729
- PMCID: PMC4464741
- DOI: 10.1212/WNL.0000000000001673
Time from convulsive status epilepticus onset to anticonvulsant administration in children
Abstract
Objective: To describe the time elapsed from onset of pediatric convulsive status epilepticus (SE) to administration of antiepileptic drug (AED).
Methods: This was a prospective observational cohort study performed from June 2011 to June 2013. Pediatric patients (1 month-21 years) with convulsive SE were enrolled. In order to study timing of AED administration during all stages of SE, we restricted our study population to patients who failed 2 or more AED classes or needed continuous infusions to terminate convulsive SE.
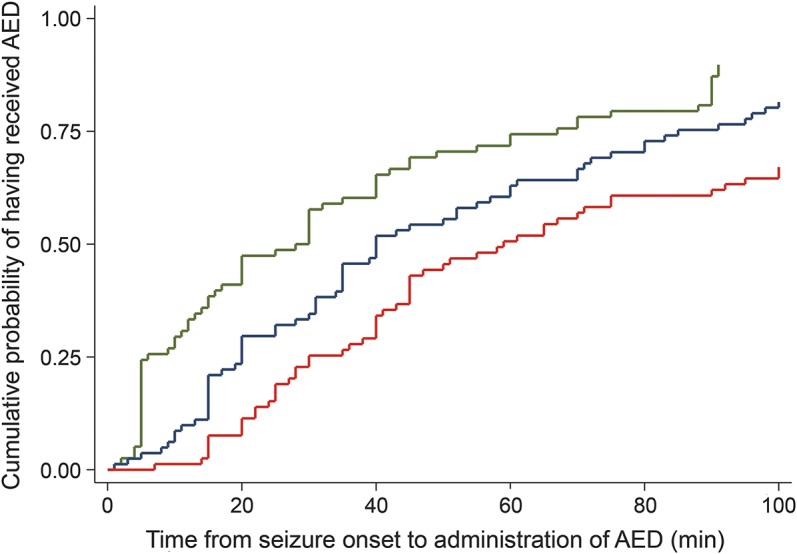
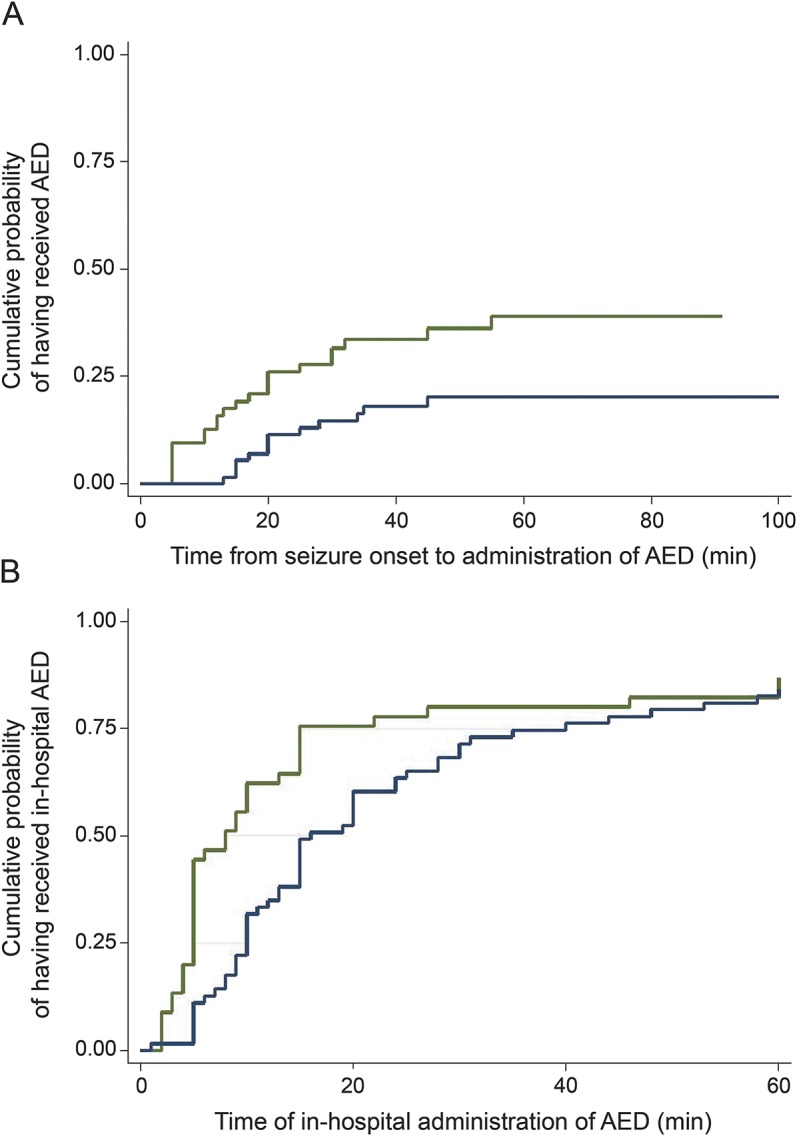
Results: We enrolled 81 patients (44 male) with a median age of 3.6 years. The first, second, and third AED doses were administered at a median (p25-p75) time of 28 (6-67) minutes, 40 (20-85) minutes, and 59 (30-120) minutes after SE onset. Considering AED classes, the initial AED was a benzodiazepine in 78 (96.3%) patients and 2 (2-3) doses of benzodiazepines were administered before switching to nonbenzodiazepine AEDs. The first and second doses of nonbenzodiazepine AEDs were administered at 69 (40-120) minutes and 120 (75-296) minutes. In the 64 patients with out-of-hospital SE onset, 40 (62.5%) patients did not receive any AED before hospital arrival. In the hospital setting, the first and second in-hospital AED doses were given at 8 (5-15) minutes and 16 (10-40) minutes after SE onset (for patients with in-hospital SE onset) or after hospital arrival (for patients with out-of-hospital SE onset).
Conclusions: The time elapsed from SE onset to AED administration and escalation from one class of AED to another is delayed, both in the prehospital and in-hospital settings.
© 2015 American Academy of Neurology.
Figures

Comment in
-
Status epilepticus: For what are we waiting?Neurology. 2015 Jun 9;84(23):2296-7. doi: 10.1212/WNL.0000000000001670. Epub 2015 May 6. Neurology. 2015. PMID: 25948730 No abstract available.
References
-
- Loddenkemper T, Goodkin HP. Treatment of pediatric status epilepticus. Curr Treat Options Neurol 2011;13:560–573. - PubMed
-
- Chin RF, Neville BG, Peckham C, Bedford H, Wade A, Scott RC. Incidence, cause, and short-term outcome of convulsive status epilepticus in childhood: prospective population-based study. Lancet 2006;368:222–229. - PubMed
-
- DeLorenzo RJ, Hauser WA, Towne AR, et al. A prospective, population-based epidemiologic study of status epilepticus in Richmond, Virginia. Neurology 1996;46:1029–1035. - PubMed
-
- Maytal J, Shinnar S, Moshe SL, Alvarez LA. Low morbidity and mortality of status epilepticus in children. Pediatrics 1989;83:323–331. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials