

Imaging in diabetic retinopathy
- PMID: 25949070
- PMCID: PMC4411609
- DOI: 10.4103/0974-9233.151887
Imaging in diabetic retinopathy
Abstract
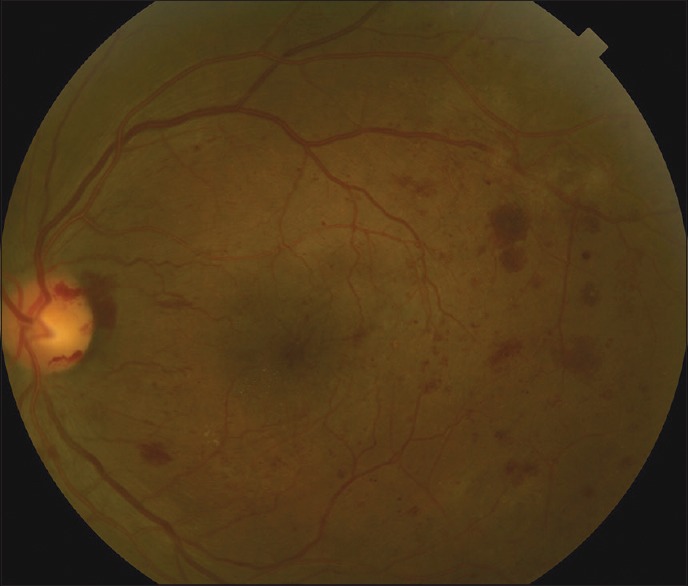
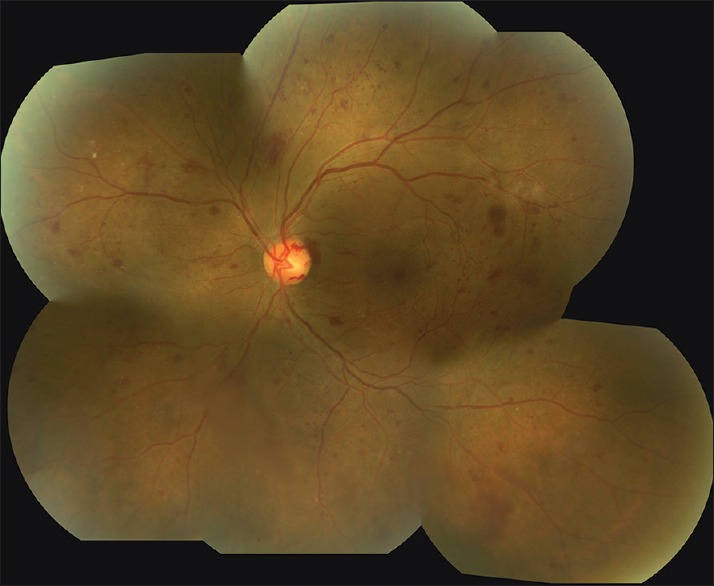
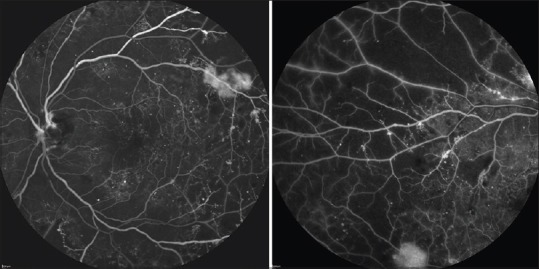
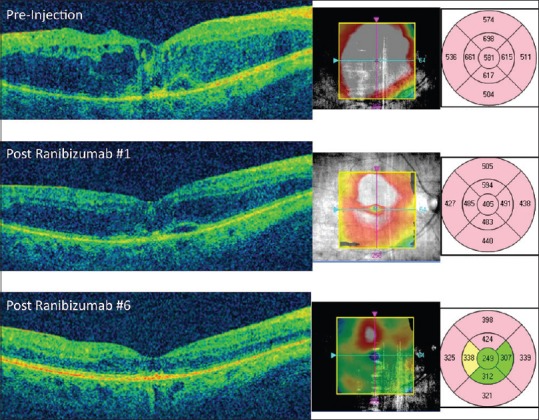
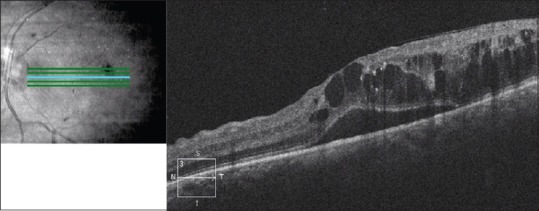
While the primary method for evaluating diabetic retinopathy involves direct and indirect ophthalmoscopy, various imaging modalities are of significant utility in the screening, evaluation, diagnosis, and treatment of different presentations and manifestations of this disease. This manuscript is a review of the important imaging modalities that are used in diabetic retinopathy, including color fundus photography, fluorescein angiography, B-scan ultrasonography, and optical coherence tomography. The article will provide an overview of these different imaging techniques and how they can be most effectively used in current practice.
Keywords: B-scan Ultrasonography; Color Fundus Photography; Diabetic Retinopathy; Fluorescein Angiography; Optical Coherence Tomography; Retinal Imaging.
Conflict of interest statement
Figures

Comment in
-
Imaging in Diabetic Retinopathy.Middle East Afr J Ophthalmol. 2015 Oct-Dec;22(4):531. doi: 10.4103/0974-9233.167809. Middle East Afr J Ophthalmol. 2015. PMID: 26692733 Free PMC article. No abstract available.
-
Author's Reply.Middle East Afr J Ophthalmol. 2015 Oct-Dec;22(4):532. Middle East Afr J Ophthalmol. 2015. PMID: 26692734 Free PMC article. No abstract available.
References
-
- Patrick JS, Tyler ME. 2nd ed. New York: Butterworth-Heinemann Medical; 2001. Fundus photography overview. Ophthalmic Photography: Retinal Photography, Angiography, and Electronic Imaging.
-
- Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report Number 2. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1987;94:761–74. - PubMed
-
- Witmer MT, Kiss S. The clinical utility of ultra-wide-field imaging. Rev Ophthalmol. 2012. [Last accessed on 2015 Jan 29]. Available from: http://www.reviewofophthalmology.com/content/d/retinal_insider/c/32799 .
-
- Tyler ME. Stereo fundus photography: Principles and technique. J Ophthalmic Photogr. 1996;18:68–89.
-
- Li HK, Hubbard LD, Danis RP, Esquivel A, Florez-Arango JF, Krupinski EA. Monoscopic versus stereoscopic retinal photography for grading diabetic retinopathy severity. Invest Ophthalmol Vis Sci. 2010;51:3184–92. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
