

US chiropractors' attitudes, skills and use of evidence-based practice: A cross-sectional national survey
- PMID: 25949800
- PMCID: PMC4422535
- DOI: 10.1186/s12998-015-0060-0
US chiropractors' attitudes, skills and use of evidence-based practice: A cross-sectional national survey
Abstract
Background: Evidence based practice (EBP) is being increasingly utilized by health care professionals as a means of improving the quality of health care. The introduction of EBP principles into the chiropractic profession is a relatively recent phenomenon. There is currently a lack of information about the EBP literacy level of US chiropractors and the barriers/facilitators to the use of EBP in the chiropractic profession.
Methods: A nationwide EBP survey of US chiropractors was administered online (Nov 2012-Mar 2013) utilizing a validated self-report instrument (EBASE) in which three sub-scores are reported: attitudes, skills and use. Means, medians, and frequency distributions for each of the sub-scores were generated. Descriptive statistics were used to analyze the demographic characteristics of the sample. Means and proportions were calculated for all of the responses to each of the questions in the survey.
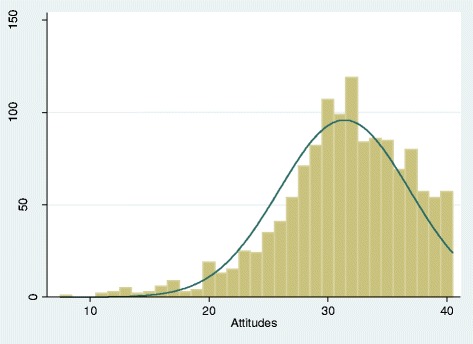
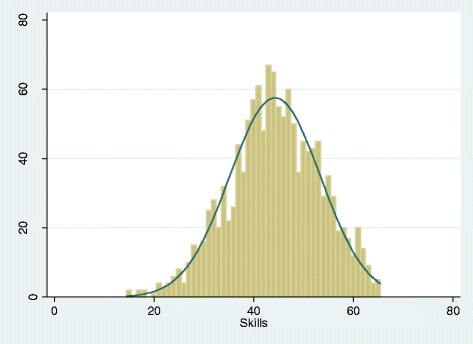
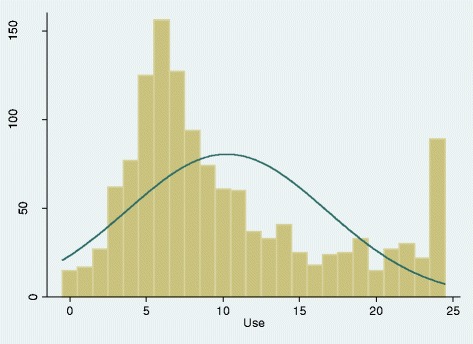
Results: A total of 1,314 US chiropractors completed the EBASE survey; the sample appeared to be representative of the US chiropractic profession. Respondents were predominantly white (94.3%), male (75%), 47 (+/- 11.6) years of age, and in practice for more than 10 years (60%). EBASE sub-score means (possible ranges) were: attitudes, 31.4 (8-40); skills, 44.3 (13-65); and use, 10.3 (0-24). Survey participants generally held favorable attitudes toward EBP, but reported less use of EBP. A minority of participants indicated that EBP coursework (17%) and critical thinking (29%) were a major part of their chiropractic education. The most commonly reported barrier to the use of EBP was "lack of time". Almost 90% of the sample indicated that they were interested in improving their EBP skills.
Conclusion: American chiropractors appear similar to chiropractors in other countries, and other health professionals regarding their favorable attitudes towards EBP, while expressing barriers related to EBP skills such as research relevance and lack of time. This suggests that the design of future EBP educational interventions should capitalize on the growing body of EBP implementation research developing in other health disciplines. This will likely include broadening the approach beyond a sole focus on EBP education, and taking a multilevel approach that also targets professional, organizational and health policy domains.
Keywords: Chiropractic; Complementary and alternative medicine; Dissemination and implementation; Evidence-based medicine; Knowledge translation; Survey research.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
