

High risk of cerebrospinal fluid leakage in surgery of a rare primary intraosseous cavernous hemangioma of the clivus showing meningeal infiltration: A case report and review of the literature
- PMID: 25949853
- PMCID: PMC4408619
- DOI: 10.4103/2152-7806.155695
High risk of cerebrospinal fluid leakage in surgery of a rare primary intraosseous cavernous hemangioma of the clivus showing meningeal infiltration: A case report and review of the literature
Abstract
Background: Primary intraosseous cavernous hemangiomas (PICH) of the skull represent an infrequent bone tumor. Although some rare cases of PICHs located in the skull base have been published, to our concern only three cases have been reported in the English literature of PICHs arising within the clivus.
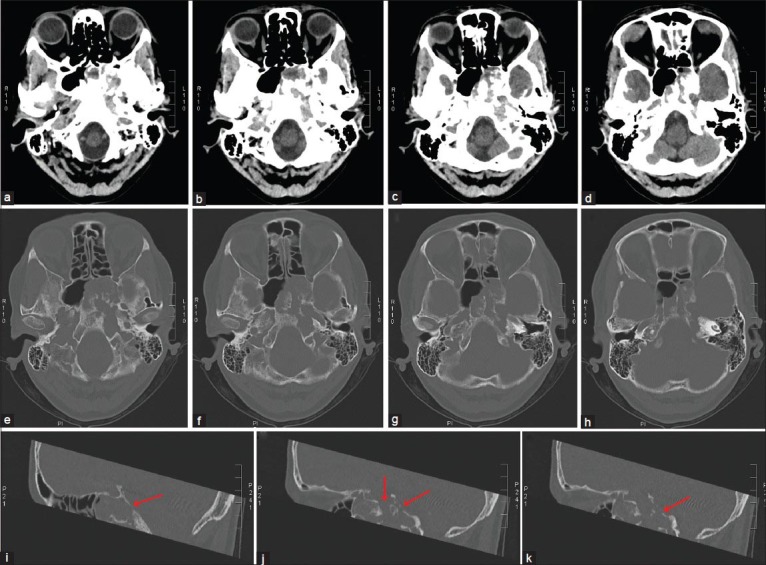
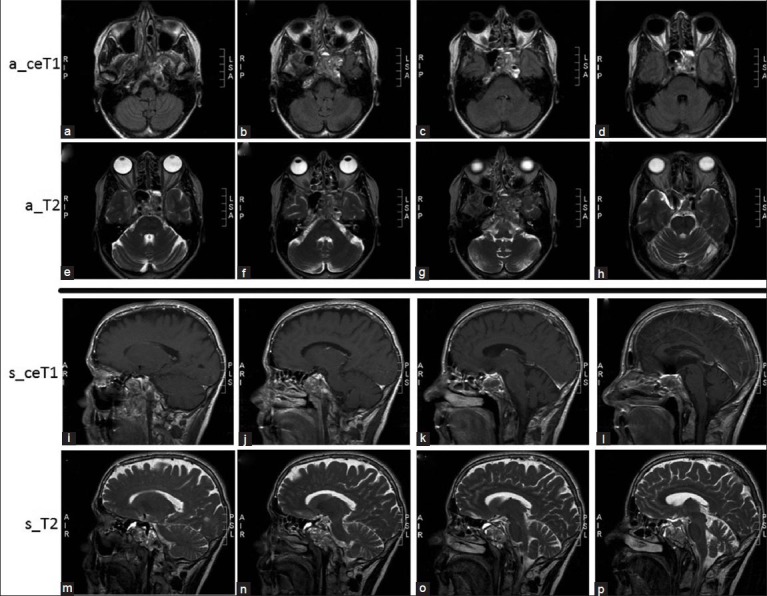
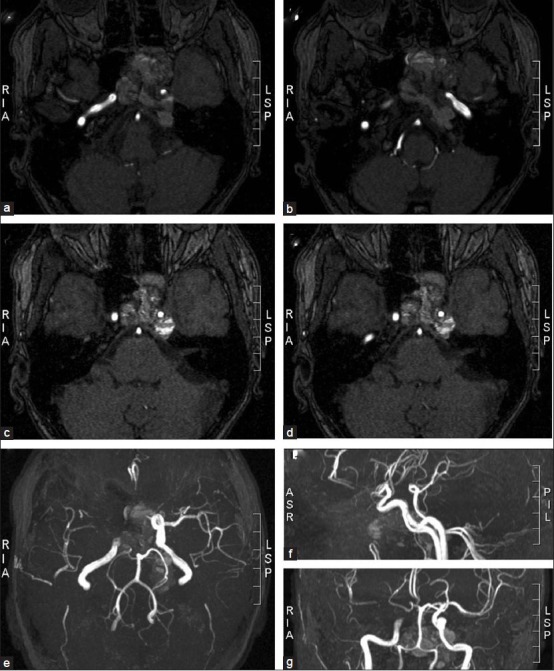
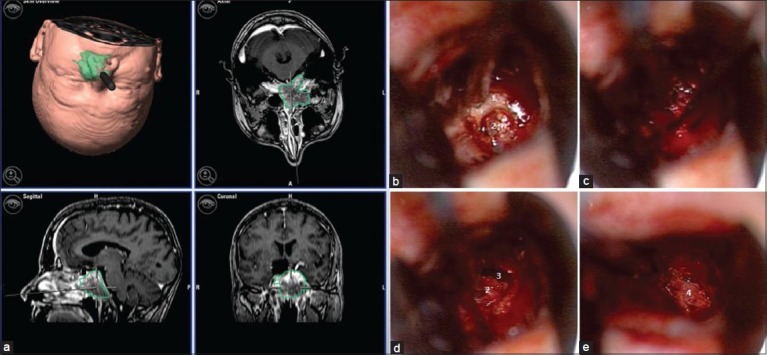
Case description: We present the case of a patient presenting an isolated abducens paresis due to a rare PICH of the clivus showing also an unusual destruction of the inner table as well as infiltration of the dura mater. Due to this uncommon infiltrative pattern of an otherwise expected intraosseous tumor, a cerebrospinal fluid (CSF)-fistula occurred while performing a transnasal biopsy. The patient recovered successfully without need of lumbar drainage or re-surgery. Additionally, intratumoral decompression was sufficient to relief the abducens paresis.
Conclusions: Our case provides new and meaningful information about clinical features as well as growth pattern of these rare clival tumors. We also discuss the importance of knowing these peculiarities before surgery in order to plan the optimal operative management as well as to avoid complications while approaching PICHs localized in such a delicate cranial region.
Keywords: Clivus; cavernous hemangioma; cerebrospinal fluid leakage.
Figures
References
-
- Banerji D, Inao S, Sugita K, Kaur A, Chhabra DK. Primary intraosseous orbital hemangioma: A case report and review of the literature. Neurosurgery. 1994;35:1131–4. - PubMed
-
- Bottrill I, Poe DS. Imaging quiz case 2. Intraosseous cavernous–type hemangioma of the petrous temporal bone. Arch Otolaryngol Head Neck Surg. 1995;121:348. 350. - PubMed
-
- Bucy PC, Capp CS. Primary hemangioma of bone with special reference to roentgenologic diagnosis. AJR Am J Roentgenol. 1930;23:1–33.
-
- Curtin HD, Jensen JE, Barnes L, Jr, May M. “Ossifying” hemangiomas of the temporal bone: Evaluation with CT. Radiology. 1987;164:831–5. - PubMed
-
- Dickins JR. Cavernous hemangioma of the sphenoid wing. Arch Otolaryngol. 1978;104:58–60. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources