

Pneumatic retinopexy versus scleral buckle for repairing simple rhegmatogenous retinal detachments
- PMID: 25950286
- PMCID: PMC4451439
- DOI: 10.1002/14651858.CD008350.pub2
Pneumatic retinopexy versus scleral buckle for repairing simple rhegmatogenous retinal detachments
Update in
-
Pneumatic retinopexy versus scleral buckle for repairing simple rhegmatogenous retinal detachments.Cochrane Database Syst Rev. 2021 Nov 11;11(11):CD008350. doi: 10.1002/14651858.CD008350.pub3. Cochrane Database Syst Rev. 2021. PMID: 34762741 Free PMC article.
Abstract
Background: Rhegmatogenous retinal detachment (RRD) is a full-thickness break in the sensory retina, caused by vitreous traction on the retina. While pneumatic retinopexy, scleral buckle, and vitrectomy are the accepted surgical interventions for eyes with RRD, their relative effectiveness has remained controversial.
Objectives: The objectives of this review were to assess the effectiveness and safety of pneumatic retinopexy versus scleral buckle or pneumatic retinopexy versus a combination treatment of scleral buckle and vitrectomy for people with RRD. The secondary objectives were to summarize any data on economic measures and quality of life.
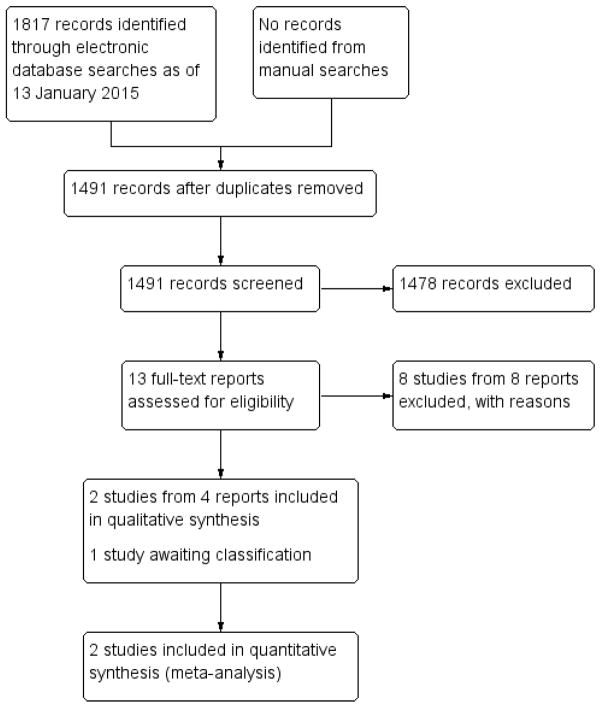
Search methods: We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (2014, Issue 12), Ovid MEDLINE, Ovid MEDLINE In-Process and Other Non-Indexed Citations, Ovid MEDLINE Daily, Ovid OLDMEDLINE (January 1946 to January 2015), EMBASE (January 1980 to January 2015), Latin American and Caribbean Health Sciences Literature Database (LILACS) (January 1982 to January 2015), the ISRCTN registry (www.isrctn.com/editAdvancedSearch), ClinicalTrials.gov (www.clinicaltrials.gov) and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not use any date or language restrictions in the electronic searches for trials. We last searched the electronic databases on 13 January 2015.
Selection criteria: We included all randomized or quasi-randomized controlled trials comparing the effectiveness of pneumatic retinopexy versus scleral buckle (with or without vitrectomy) for eyes with RRD.
Data collection and analysis: After screening for eligibility, two review authors independently extracted study characteristics, methods, and outcomes. We followed systematic review standards as set forth by The Cochrane Collaboration.
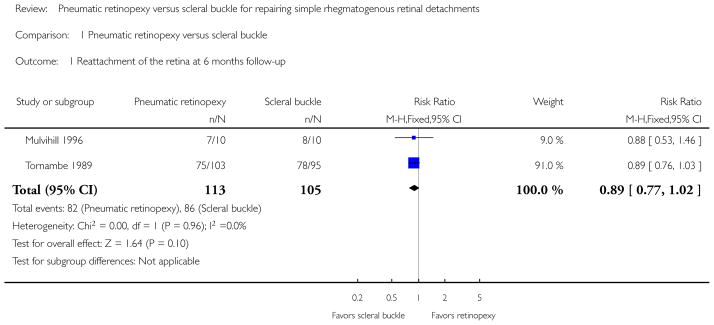
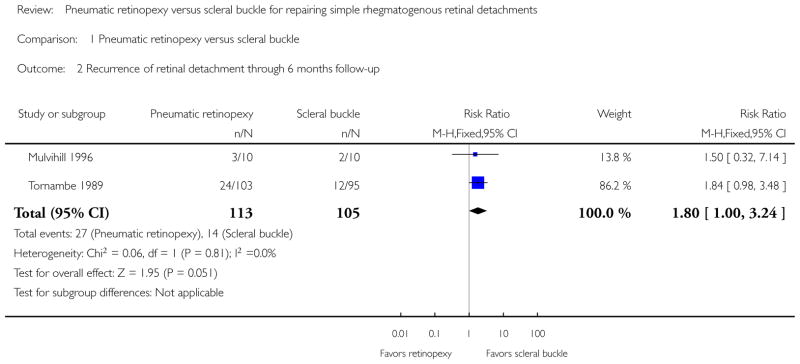
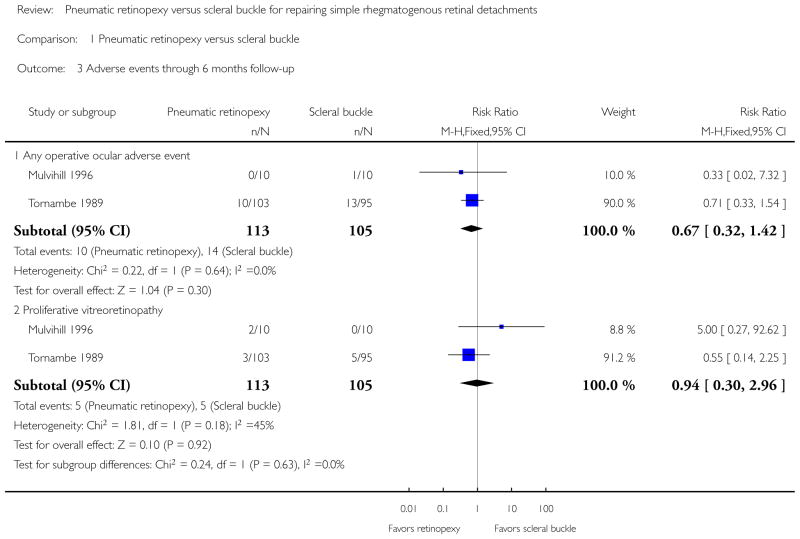
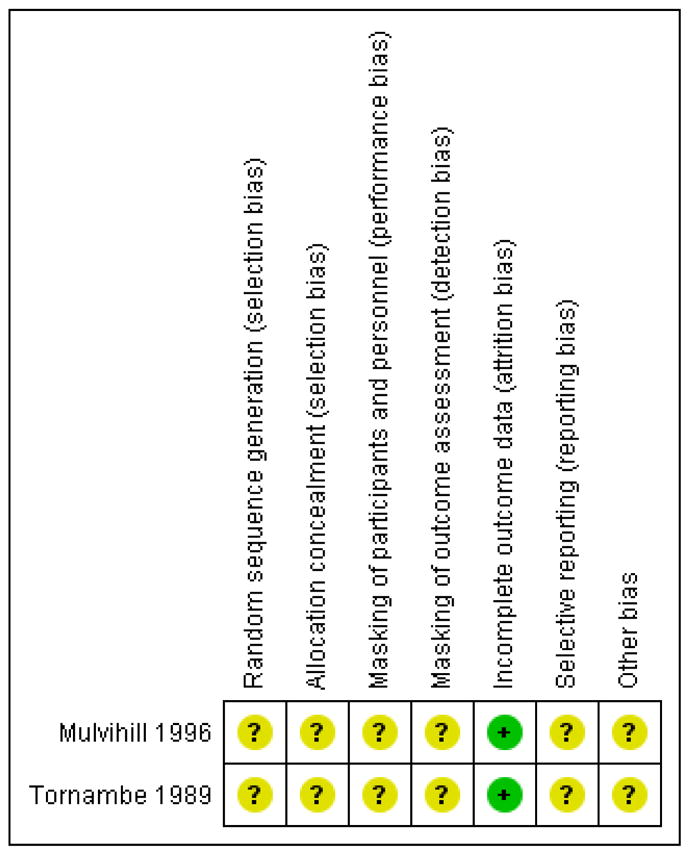
Main results: We included two randomized controlled trials (218 eyes of 216 participants) comparing the effectiveness of pneumatic retinopexy versus scleral buckle for eyes with RRD. We identified no studies investigating the comparison of pneumatic retinopexy versus a combination treatment of scleral buckle and vitrectomy. Of the two included studies, one was a small study with 20 participants enrolled in Ireland and followed for an average of 16 months. The second study was larger with 196 participants (198 eyes) enrolled in the United States and followed for at least 6 months. Cautious interpretation of the results is warranted, since we graded the evidence as low to moderate quality due to insufficient reporting of study methods and imprecision and inconsistency among study results.Both studies showed fewer eyes achieving retinal reattachment in the pneumatic retinopexy group compared with the scleral buckle group by six-months follow-up (risk ratio (RR) 0.89, 95% confidence interval (CI) 0.77 to 1.02, 218 eyes); however, we are uncertain as to whether the intervention has an important effect on reattachment because the results are imprecise. Eyes in the pneumatic retinopexy group also were more likely to have had a recurrence of retinal detachment by six-months follow-up (RR 1.80, 95% CI 1.00 to 3.24, 218 eyes); however, we are uncertain as to whether the intervention has an important effect on recurrence because the lower CI equals no difference. Neither study reported mean change in visual acuity, quality of life data, or economic measures. Differences between the pneumatic retinopexy group and scleral buckle group were uncertain due to small numbers of events with respect to operative ocular adverse events (RR 0.67, 95% CI 0.32 to 1.42, 218 eyes), development of cataract (RR 0.92, 95% CI 0.06 to 14.54, 198 eyes), glaucoma (RR 0.31, 95% CI 0.03 to 2.91, 198 eyes), macular pucker (RR 0.74, 95% CI 0.20 to 2.67, 198 eyes), and proliferative vitreoretinopathy (RR 0.94, 95% CI 0.30 to 2.96, 218 eyes). Fewer eyes in the pneumatic retinopexy group compared with the scleral buckle group experienced choroidal detachment (RR 0.17, 95% CI 0.05 to 0.57, 198 eyes) or myopic shift equal to or greater than 1 diopter spherical equivalent (RR 0.04, 95% CI 0.01 to 0.13, 198 eyes).
Authors' conclusions: The evidence suggests that pneumatic retinopexy may result in lower rates of reattachment and higher rates of recurrence than scleral buckle for eyes with RRD, but does not rule out no difference between procedures. The relative safety of the procedures is uncertain and the relative effects of these procedures in terms of other patient-important outcomes, such as visual acuity and quality of life, is unknown. Due to the limited information available between pneumatic retinopexy and scleral buckle procedures, future research addressing these evidence gaps are warranted.
Figures
References
References to studies included in this review
-
- Mulvihill A, Fulcher T, Datta V, Acheson R. Pneumatic retinopexy versus scleral buckling: a randomised controlled trial. Irish Journal of Medical Science. 1996;165(4):274–7. - PubMed
-
- Tornambe PE, Hilton GF. Pneumatic retinopexy. A multicenter randomized controlled clinical trial comparing pneumatic retinopexy with scleral buckling. The Retinal Detachment Study Group. Ophthalmology. 1989;96(6):772–83. - PubMed
- Tornambe PE, Hilton GF, Brinton DA, Flood TP, Green S, Grizzard WS, et al. Pneumatic retinopexy. A two-year follow-up study of the multicenter clinical trial comparing pneumatic retinopexy with scleral buckling. Ophthalmology. 1991;98(7):1115–23. - PubMed
- Tornambe PE, Hilton GF, Grizzard WS, Hammer ME, Poliner LS, Yarian DL, et al. Pneumatic retinopexy: a two-year randomized controlled follow-up study comparing pneumatic retinopexy with scleral buckling. American Academy of Ophthalmology. 1990;123
References to studies excluded from this review
-
- Avitabile T, Bartolotta G, Torrisi B, Reibaldi A. A randomized prospective study of rhegmatogenous retinal detachment cases treated with cryopexy versus frequency-doubled Nd:YAG laser-retinopexy during episcleral surgery. Retina. 2004;24(6):878–82. - PubMed
-
- Barr CC. Pneumatic retinopexy and balloon buckles as alternatives to conventional scleral buckling surgery. Seminars in Ophthalmology. 1995;10(1):2–8. - PubMed
-
- Figueroa M, Schirru A, Corte MD, Sbordone S, Romano A. Scleral buckling technique without retinopexy for treatment of rhegmatogenous retinal detachment. American Academy of Ophthalmology. 2000:123. - PubMed
-
- Hsu J, Gerstenblith AT, London NJ, Garg SJ, Spirn MJ, Maguire JI, et al. Effect of topical aqueous suppression on intraocular gas duration after pure perfluoropropane injection in nonvitrectomized eyes with retinal detachment. Retina. 2014;34(12):2458–61. - PubMed
-
- Maia OO, Jr, Takahashi WY, Chizzotti Bonanomi MT, Arantes TE. Rhegmatogenous retinal detachment: a postoperative study of the macula [Descolamento regmatogênico de retina: avaliação pós–operatória da mácula] Arquivos Brasileiros de Oftalmologia. 2007;70(6):996–1000. - PubMed
References to studies awaiting assessment
-
- Betran-Loustaunau MA, Troconis D, Morales-Canton V, Ochoa-Contreras D, Dalma-Weiszhausz J, Jimenez-Sierra JM, et al. Comparative study of vitrectomy, pneumatic retinopexy, and scleral buckling for primary rhegmatogenous retinal-detachment. Investigative Ophthalmology and Visual Science. 1997 ARVO E-Abstract 3156.
Additional references
-
- American Academy of Ophthalmology. The repair of rhegmatogenous retinal detachments. A report by the American Academy of Ophthalmology Committee on Ophthalmic Procedure Assessment Ophthalmology. 1996;103(8):1313–24. - PubMed
-
- Algvere PV, Jahnberg P, Textorius O. The Swedish Retinal Detachment Register. I. A database for epidemiological and clinical studies. Graefe’s Archive for Clinical and Experimental Ophthalmology. 1999;237(2):137–44. - PubMed
-
- Byer NE. What happens to untreated asymptomatic retinal breaks, and are they affected by posterior vitreous detachment? Ophthalmology. 1998;105(6):1045–50. - PubMed
-
- Deeks JJ, Higgins JPT, Altman DG, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration; 2011. Chapter 9: Analysing data and undertaking meta-analyses. Version 5.1.0 [updated March 2011] Available from www.cochrane-handbook.org.
References to other published versions of this review
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials