

Fatty lesions in and around the heart: a pictorial review
- PMID: 25950727
- PMCID: PMC4628539
- DOI: 10.1259/bjr.20150157
Fatty lesions in and around the heart: a pictorial review
Abstract
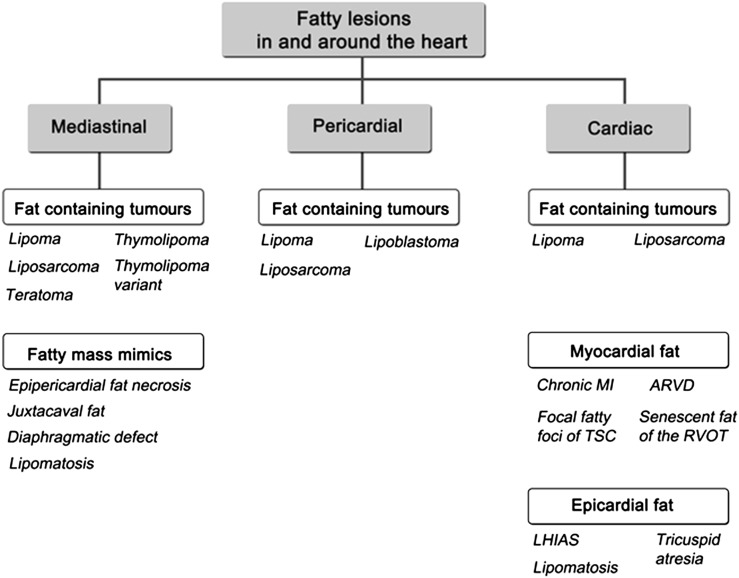
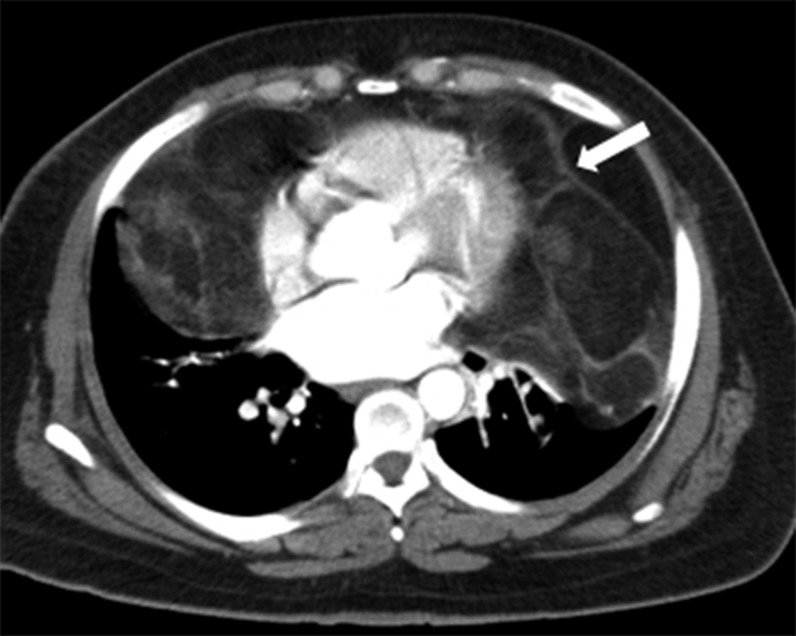
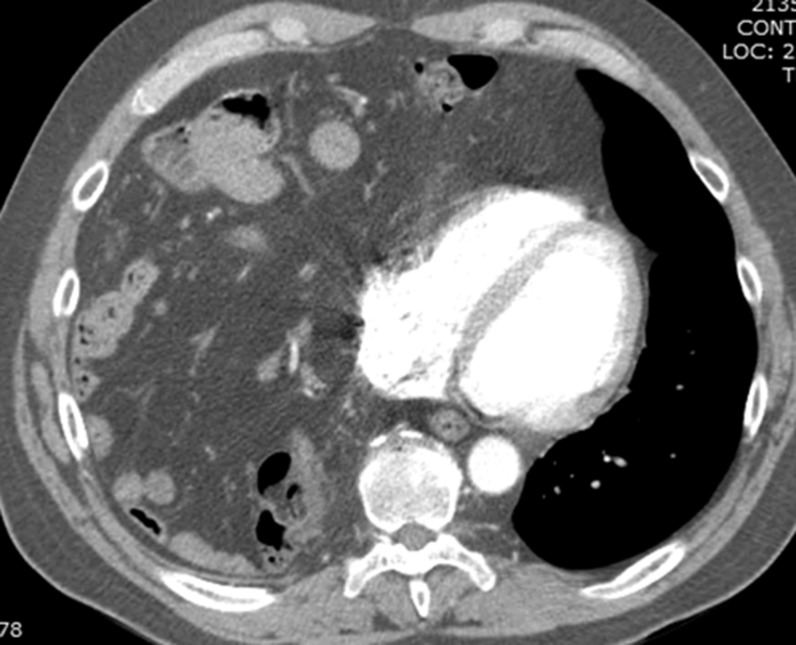
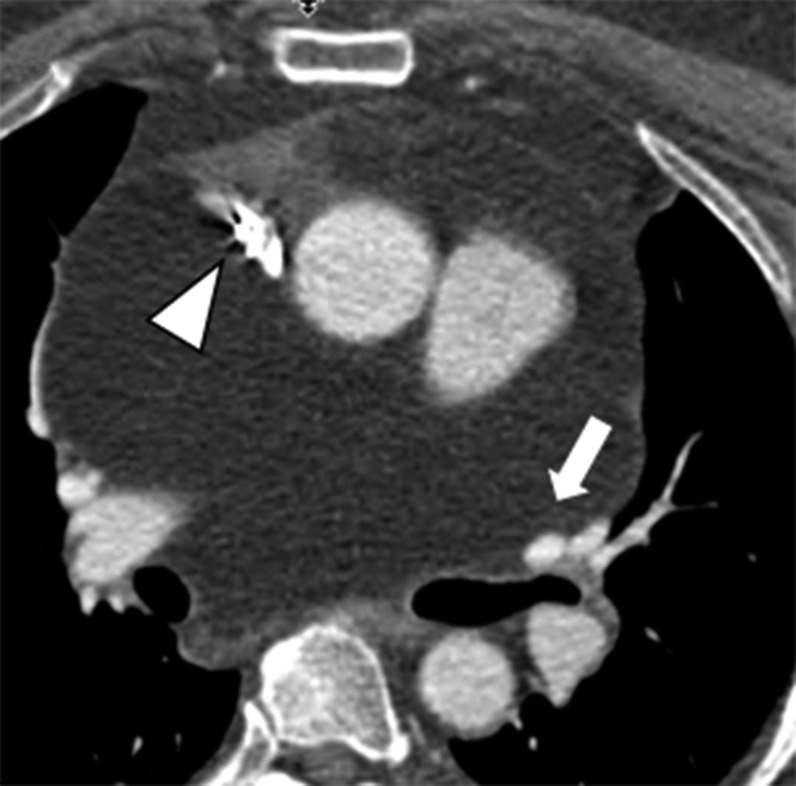
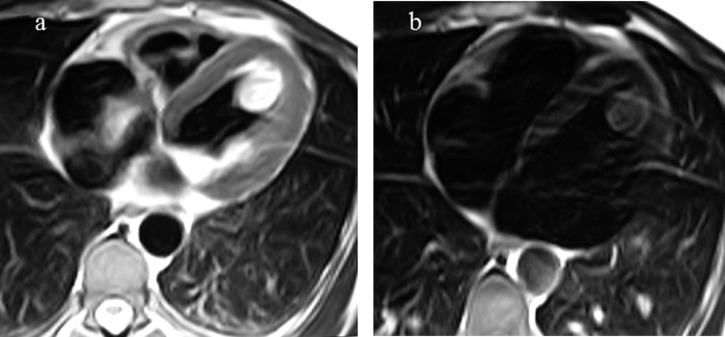
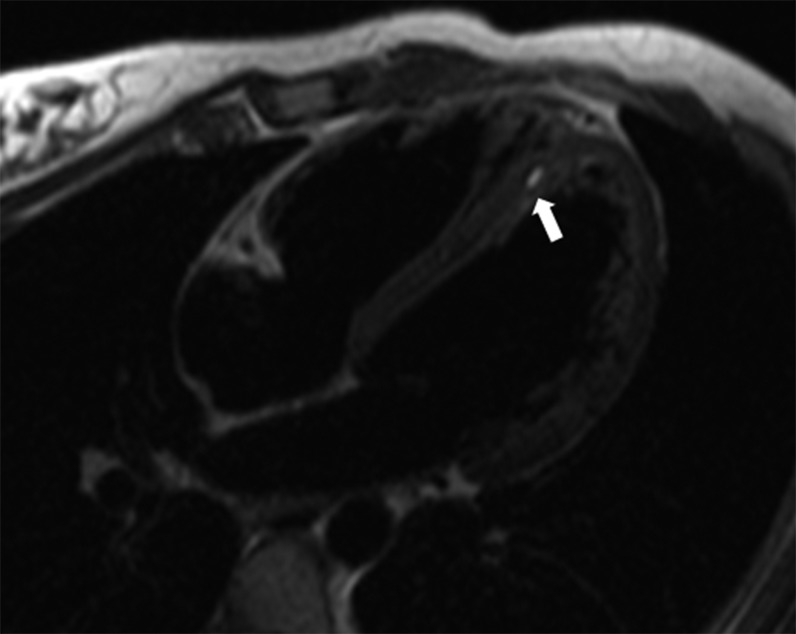
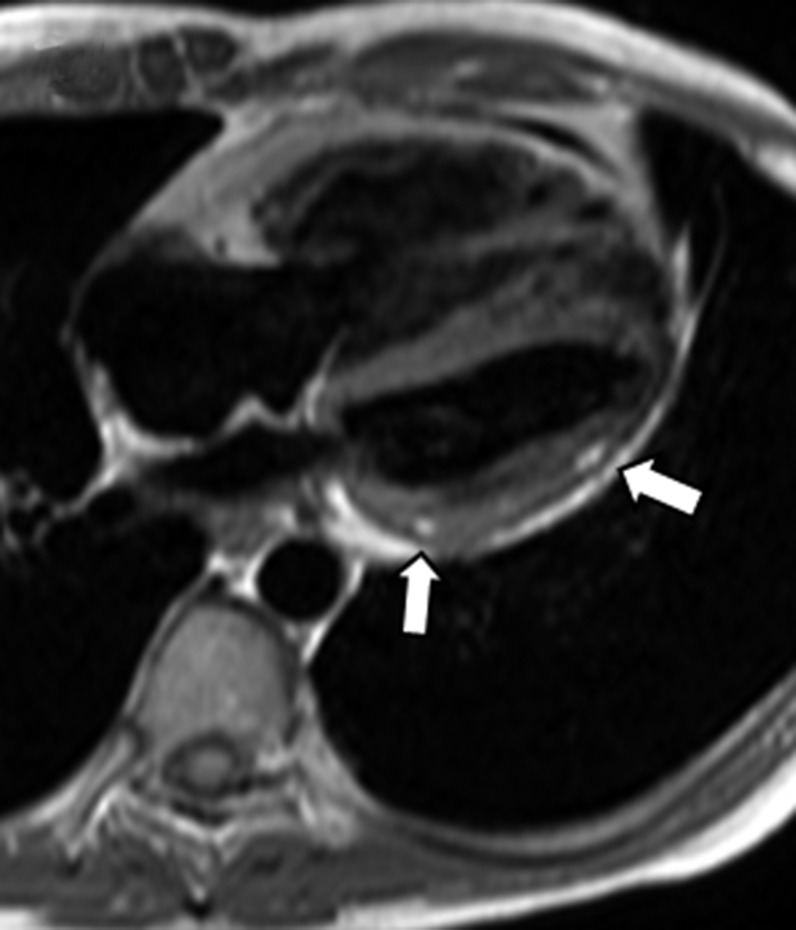
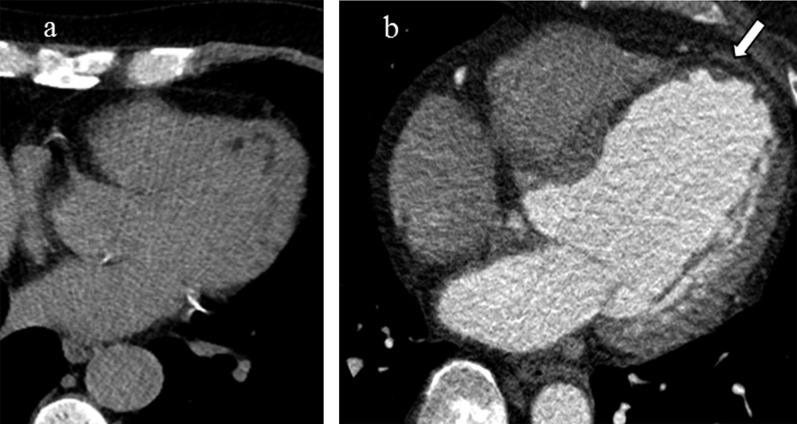
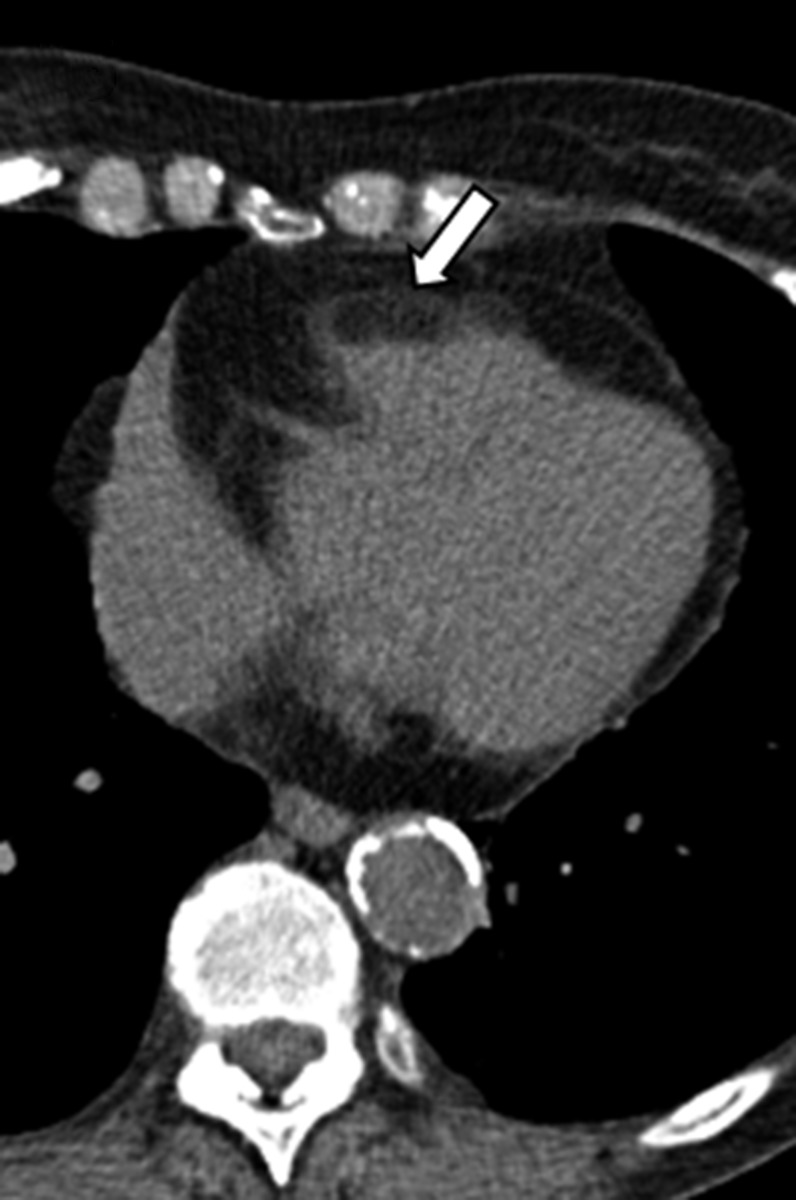
A wide variety of fat-containing entities occur in and near the heart. These findings are often encountered by radiologists and may be incidental or the reason for the patient's clinical presentation. Cross-sectional imaging helps to characterize the extent of these lesions and to formulate a differential diagnosis, which varies by lesion location, imaging features and patient demographics. The purpose of this pictorial essay is to familiarize radiologists with these fat-containing lesions and to help avoid misdiagnosis and errors in management. This pictorial review will discuss the normal fatty structures in and around the heart. A range of common and uncommon fat-containing lesions will then be reviewed based upon lesion location.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
