

Optimizing atrial fibrillation management: from ICU and beyond
- PMID: 25951122
- PMCID: PMC4594627
- DOI: 10.1378/chest.15-0358
Optimizing atrial fibrillation management: from ICU and beyond
Abstract
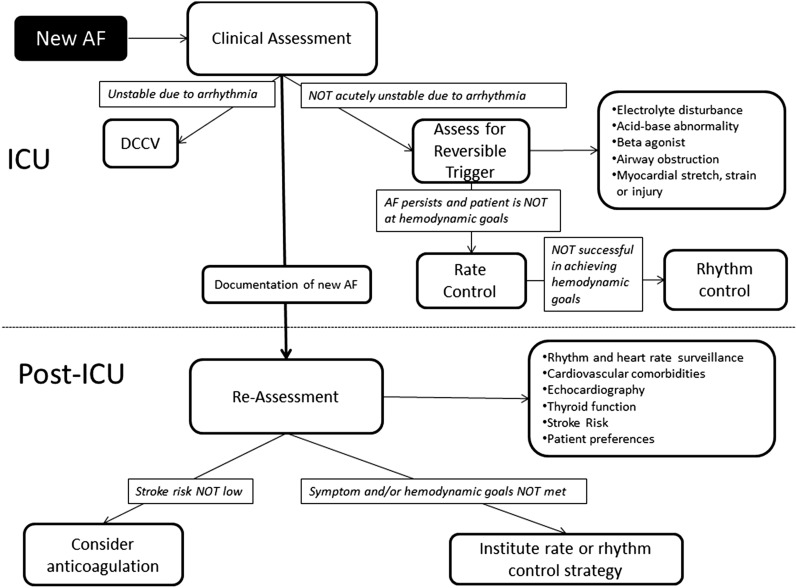
Atrial fibrillation (AF) that newly occurs during critical illness presents challenges for both short- and long-term management. During critical illness, patients with new-onset AF are clinically evaluated for hemodynamic instability owing to the arrhythmia as well as for potentially reversible arrhythmia triggers. Hemodynamically significant AF that persists during critical illness may be treated with heart rate or rhythm control strategies. Recent evidence suggests that patients in whom AF develops during acute illness (eg, sepsis, postoperatively) have high long-term risks for AF recurrence and for AF-associated complications, such as stroke, heart failure, and death. Therefore, we suggest increased efforts to improve communication of AF events between inpatient and outpatient providers and to reassess patients who had experienced new-onset AF during critical illness after they transition to the post-ICU setting. We describe various strategies for the assessment and long-term management of patients with new-onset AF during critical illness.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
