

Comparison of two different mechanical esophagogastric anastomosis in esophageal cancer patients: a meta-analysis
- PMID: 25952323
- PMCID: PMC4456702
- DOI: 10.1186/s13019-015-0271-4
Comparison of two different mechanical esophagogastric anastomosis in esophageal cancer patients: a meta-analysis
Abstract
Objective: In this meta-analysis, we conducted a pooled analysis of clinical studies comparing Linear Stapled (LS) versus Circular Stapled (CS) esophagogastric anastomosis for esophageal cancer.
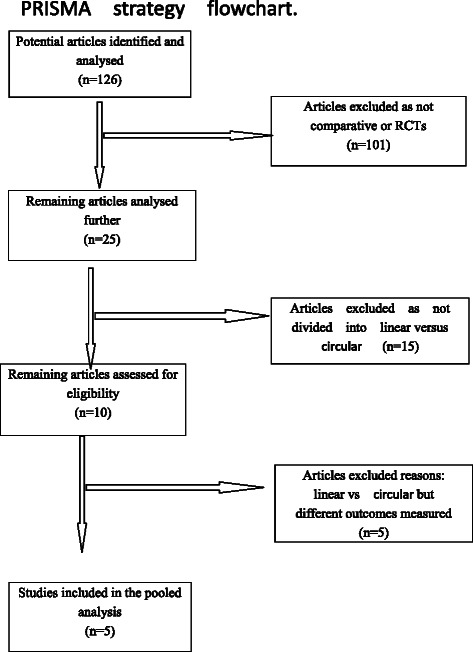
Methods: According to the recommendations of the Cochrane Collaboration, we established a rigorous study protocol. We performed a systematic electronic search of the PubMed, Embase, Cochrane Library, Web of Science, and Chinese Biomedical databases as well as Chinese scientific journals to identify articles to include in our meta-analysis. The primary outcomes compared were anastomotic leak, anastomotic stricture and 3-month mortality.
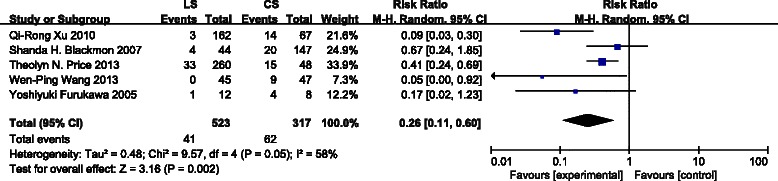
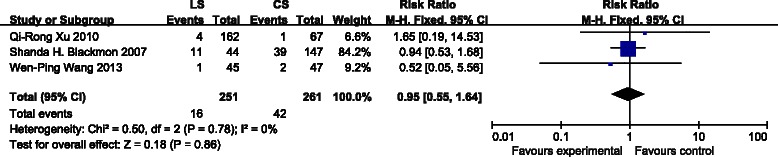
Results: Five controlled trials comprising 840 patients (523 LS vs. 317 CS) were included. Primary outcomes revealed a statistically significant decrease in anastomotic strictures [risk ratio (RR): 0.26, 95 % confidence interval (CI): 0.11-0.60, P = 0.002] compared with linear stapled anastomosis. However, there were no significant differences between the two groups with respect to anastomotic leakage [risk ratio (RR): 0.80, 95 % confidence interval (CI): 0.40-1.58, P = 0.52] and 3-month mortality [risk ratio (RR): 0.94, 95 % confidence interval (CI): 0.47-1.87, P = 0.85].
Conclusion: There were no statistical differences in the rate of 3-month mortality or anastomotic leakage between the two groups. However, the LS method contributed to a reduced rate of anastomotic strictures. This meta-analysis may offer some specific suggestions for esophagogastric anastomosis.
Figures

References
-
- Biere SS, van Berge HM, Maas KW, Bonavina L, Rosman C, Garcia JR, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet. 2012;379(9829):1887–92. - PubMed
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. - PubMed
-
- Honda M, Kuriyama A, Noma H, Nunobe S, Furukawa TA. Hand-sewn versus mechanical esophagogastric anastomosis after esophagectomy: a systematic review and meta-analysis. Ann Surg. 2013;257(2):238–48. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
