

Maternal salt and fat intake causes hypertension and sustained endothelial dysfunction in fetal, weanling and adult male resistance vessels
- PMID: 25953742
- PMCID: PMC4424661
- DOI: 10.1038/srep09753
Maternal salt and fat intake causes hypertension and sustained endothelial dysfunction in fetal, weanling and adult male resistance vessels
Abstract
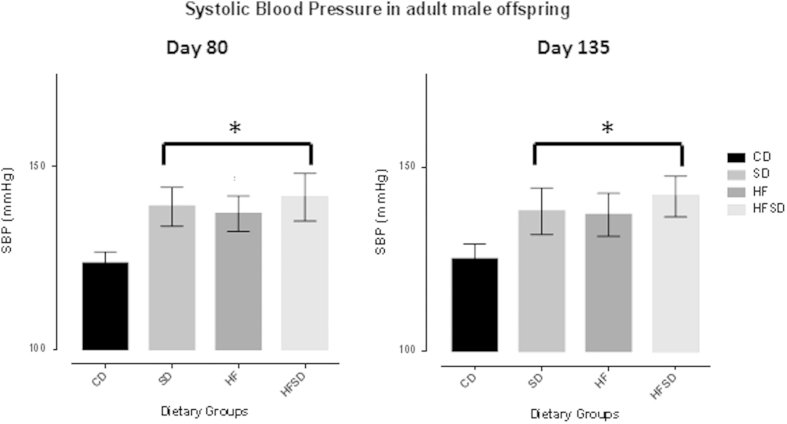
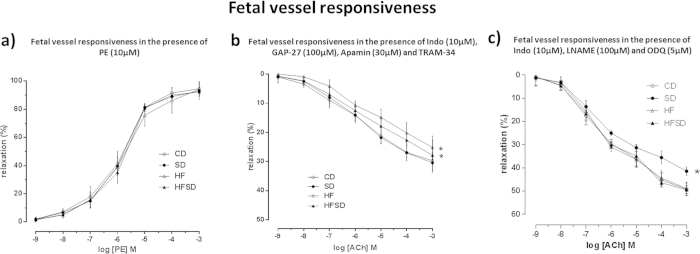
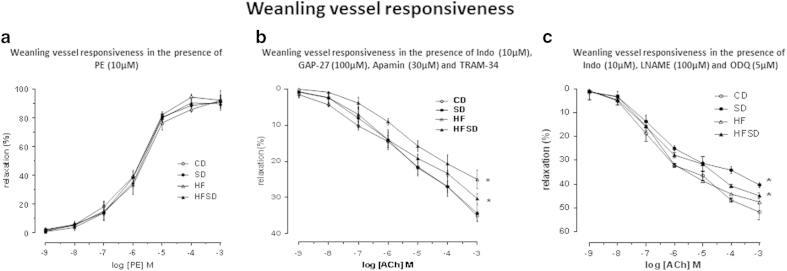
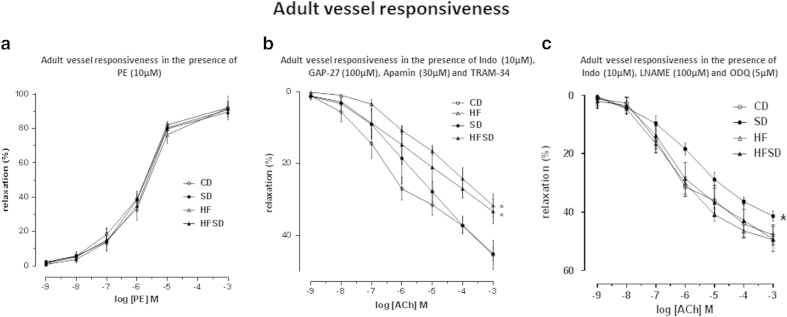
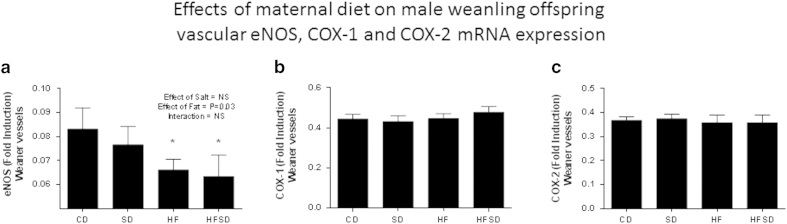
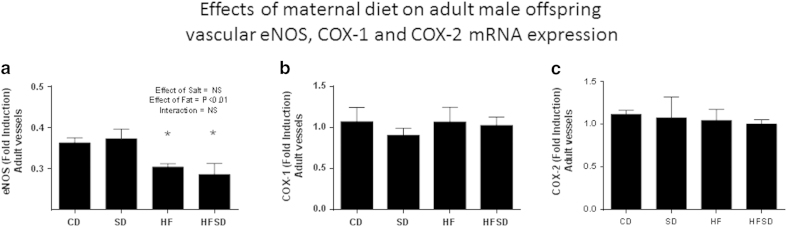
Maternal salt and fat intake can independently programme adult cardiovascular status, increasing risk of cardiovascular disease in offspring. Despite its relevance to modern western-style dietary habits, the interaction between increased maternal salt and fat intake has not been examined. Female virgin Sprague-Dawley rats were fed, a standard control diet (CD) (10% kcal fat, 1% NaCl), High-fat diet (HF) (45% kcal fat, 1% NaCl), High-salt diet (SD) (10% kcal fat, 4% NaCl), High-fat high-salt diet (HFSD) (45% kcal fat, 4% NaCl) prior to pregnancy, during pregnancy and throughout lactation. Fetal, weanling and adult vessels were mounted on a pressure myograph at fetal day 18, weaning day 21 and day 135 of adulthood. Increased blood pressure in SD, HFD and HFSD male offspring at day 80 and 135 of age was consistent with perturbed vascular function in fetal, weanling and adult vessels. Maternal salt intake reduced EDHF and calcium-mediated vasodilation, maternal fat reduced NO pathways and maternal fat and salt intake, a combination of the two pathways. Adult offspring cardiovascular disease risk may, in part, relate to vascular adaptations caused by maternal salt and/or fat intake during pregnancy, leading to persistent vascular dysfunction and sustained higher resting blood pressure throughout life.
Figures
Similar articles
-
A maternal high fat diet programmes endothelial function and cardiovascular status in adult male offspring independent of body weight, which is reversed by maternal conjugated linoleic acid (CLA) supplementation.PLoS One. 2015 Feb 19;10(2):e0115994. doi: 10.1371/journal.pone.0115994. eCollection 2015. PLoS One. 2015. PMID: 25695432 Free PMC article.
-
Excess maternal salt or fructose intake programmes sex-specific, stress- and fructose-sensitive hypertension in the offspring.Br J Nutr. 2016 Feb 28;115(4):594-604. doi: 10.1017/S0007114515004936. Epub 2015 Dec 10. Br J Nutr. 2016. PMID: 26653028
-
Predictive adaptive responses to maternal high-fat diet prevent endothelial dysfunction but not hypertension in adult rat offspring.Circulation. 2004 Aug 31;110(9):1097-102. doi: 10.1161/01.CIR.0000139843.05436.A0. Epub 2004 Aug 23. Circulation. 2004. PMID: 15326063
-
Salt intake, endothelial dysfunction, and salt-sensitive hypertension.J Clin Hypertens (Greenwich). 2002 Jan-Feb;4(1):41-6. doi: 10.1111/j.1524-6175.2002.00503.x. J Clin Hypertens (Greenwich). 2002. PMID: 11821636 Free PMC article. Review.
-
Vascular consequences of dietary salt intake.Am J Physiol Renal Physiol. 2009 Aug;297(2):F237-43. doi: 10.1152/ajprenal.00027.2009. Epub 2009 Apr 1. Am J Physiol Renal Physiol. 2009. PMID: 19339634 Free PMC article. Review.
Cited by
-
Transition in the mechanism of flow-mediated dilation with aging and development of coronary artery disease.Basic Res Cardiol. 2017 Jan;112(1):5. doi: 10.1007/s00395-016-0594-x. Epub 2016 Dec 19. Basic Res Cardiol. 2017. PMID: 27995364 Free PMC article.
-
The Double-Edged Sword Effects of Maternal Nutrition in the Developmental Programming of Hypertension.Nutrients. 2018 Dec 4;10(12):1917. doi: 10.3390/nu10121917. Nutrients. 2018. PMID: 30518129 Free PMC article. Review.
-
Maternal High-Fat and High-Salt Diets Have Differential Programming Effects on Metabolism in Adult Male Rat Offspring.Front Nutr. 2018 Mar 7;5:1. doi: 10.3389/fnut.2018.00001. eCollection 2018. Front Nutr. 2018. PMID: 29564328 Free PMC article.
-
Maternal high-fat diet increases vascular contractility in adult offspring in a sex-dependent manner.Hypertens Res. 2021 Jan;44(1):36-46. doi: 10.1038/s41440-020-0519-9. Epub 2020 Jul 27. Hypertens Res. 2021. PMID: 32719462
-
Anterior Circulation Acute Ischemic Stroke in the Plateau of China: Risk Factors and Clinical Characteristics.Front Neurol. 2022 Apr 13;13:859616. doi: 10.3389/fneur.2022.859616. eCollection 2022. Front Neurol. 2022. PMID: 35493834 Free PMC article.
References
-
- World Health Organization. A global brief on hypertension. Silent killer, global public health crisis. Geneva: World Health Organization, 2013).
-
- Ezzati M. & Riboli E. Behavioral and Dietary Risk Factors for Non-communicable Diseases N Engl J Med 369, 954–964 (2013). - PubMed
-
- Vasileska A. & Rechkoska G. Procedia. Global and Regional Food Consumption Patterns and Trends–Social and Behavioral Sciences 44, 363–369 (2012).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
