

Transmedullary Venous Anastomoses: Anatomy and Angiographic Visualization Using Flat Panel Catheter Angiotomography
- PMID: 25953764
- PMCID: PMC7965286
- DOI: 10.3174/ajnr.A4302
Transmedullary Venous Anastomoses: Anatomy and Angiographic Visualization Using Flat Panel Catheter Angiotomography
Abstract
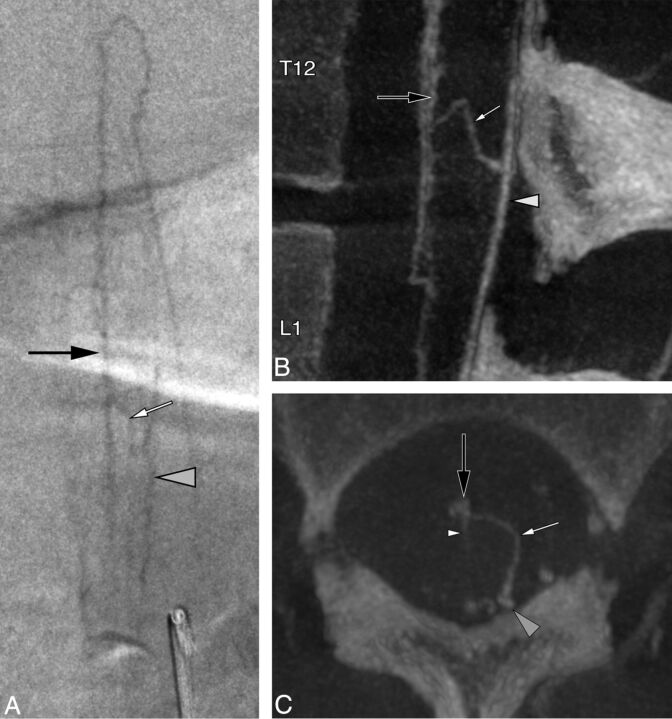
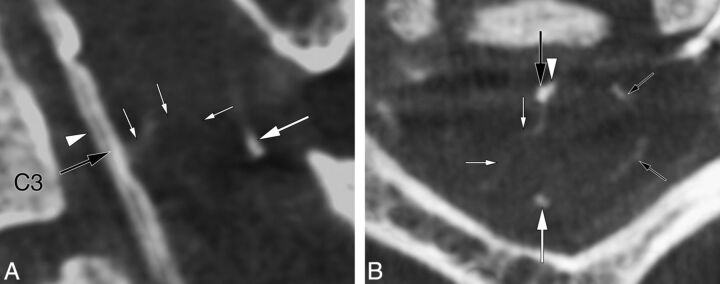
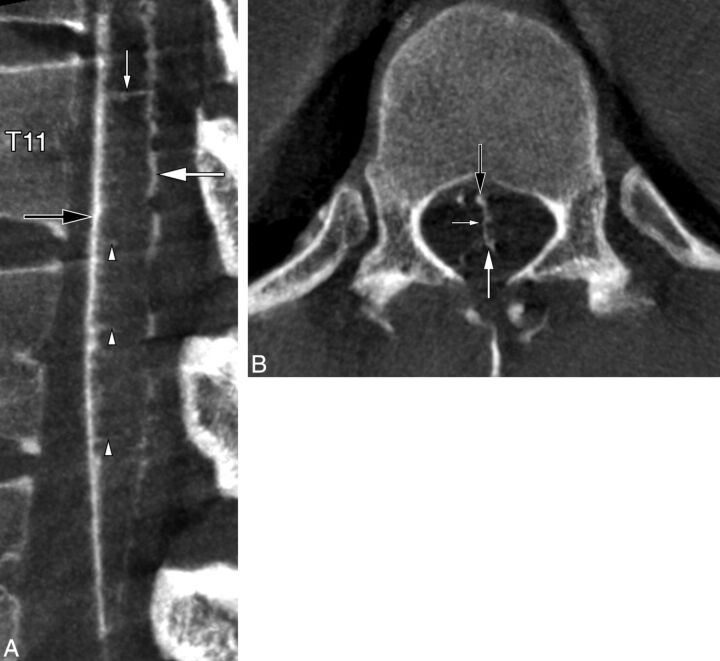
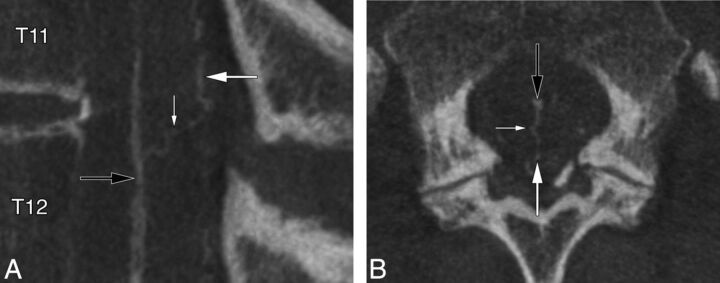
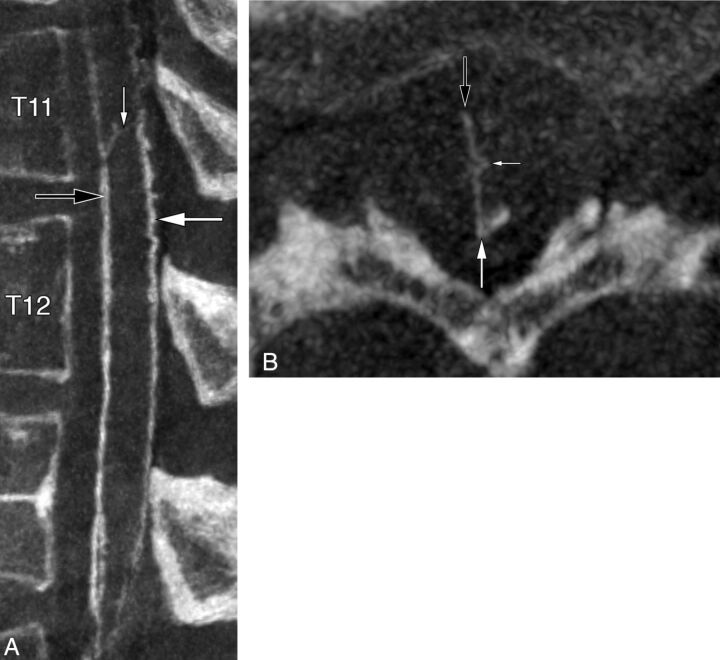
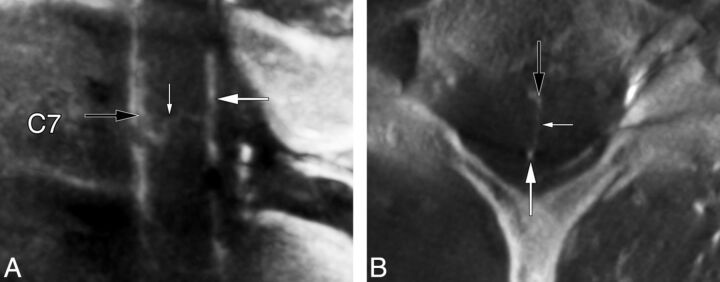
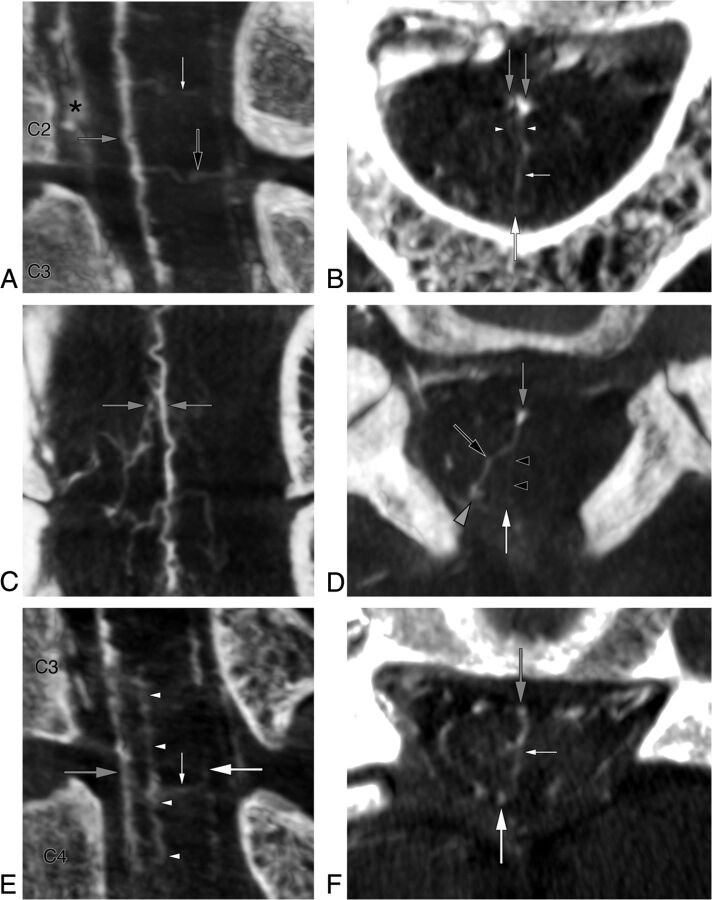
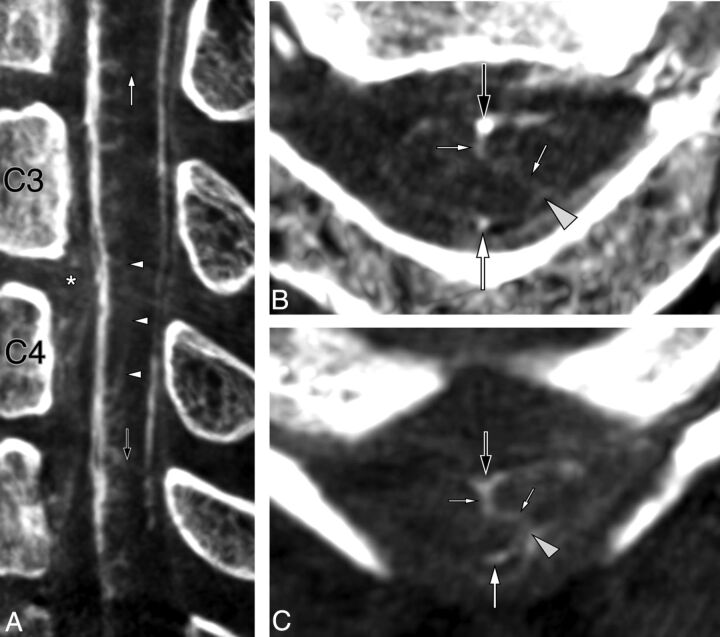
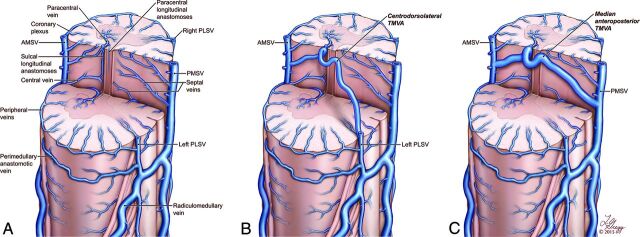
Flat panel catheter angiotomography, a recently developed angiographic technique, offers a spinal equivalent to the venous phase obtained during cerebral angiography. This report of 8 clinical cases discusses the flat panel catheter angiotomography appearance of a type of spinal venous structure until now principally known through the analysis of postmortem material, transmedullary venous anastomosis. The illustrated configurations include centrodorsolateral, median anteroposterior, median anteroposterior with duplicated origin, and combined centrodorsolateral/median anteroposterior transmedullary venous anastomoses, while a pathologic example documents the potential role of transmedullary venous anastomoses as collateral venous pathways. Two of the reported configurations have not been previously documented. Transmedullary venous anastomoses are normal venous structures that need to be differentiated from spinal cord anomalies, such as intramedullary vascular malformations.
© 2015 by American Journal of Neuroradiology.
Figures
References
-
- Akpek S, Brunner T, Benndorf G, et al. Three-dimensional imaging and cone beam volume CT in C-arm angiography with flat panel detector. Diagn Interv Radiol 2005;11:10–13 - PubMed
-
- Zellerhoff M, Scholz B, Ruehrnschopf EP, et al. Low contrast 3D reconstruction from C-arm data. SPIE Proceedings 2005;5745:646–55
-
- Pearl MS, Chen JX, Gregg L, et al. Angiographic detection and characterization of “cryptic venous anomalies” associated with spinal cord cavernous malformations using flat-panel catheter angiotomography. Neurosurgery 2012;71:125–32 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources