

Transvaginal cholecystectomy vs conventional laparoscopic cholecystectomy for gallbladder disease: A meta-analysis
- PMID: 25954114
- PMCID: PMC4419081
- DOI: 10.3748/wjg.v21.i17.5393
Transvaginal cholecystectomy vs conventional laparoscopic cholecystectomy for gallbladder disease: A meta-analysis
Abstract
Aim: To compare the results of transvaginal cholecystectomy (TVC) and conventional laparoscopic cholecystectomy (CLC) for gallbladder disease.
Methods: We performed a literature search of PubMed, EMBASE, Ovid, Web of Science, Cochrane Library, Google Scholar, MetaRegister of Controlled Trials, Chinese Medical Journal database and Wanfang Data for trials comparing outcomes between TVC and CLC. Data were extracted by two authors. Mean difference (MD), standardized mean difference (SMD), odds ratios and risk rate with 95%CIs were calculated using fixed- or random-effects models. Statistical heterogeneity was evaluated with the χ(2) test. The fixed-effects model was used in the absence of statistically significant heterogeneity. The random-effects model was chosen when heterogeneity was found.
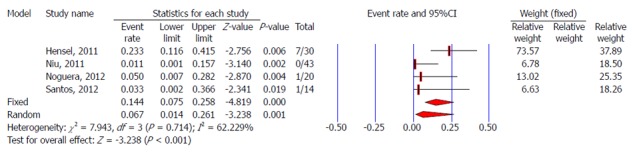
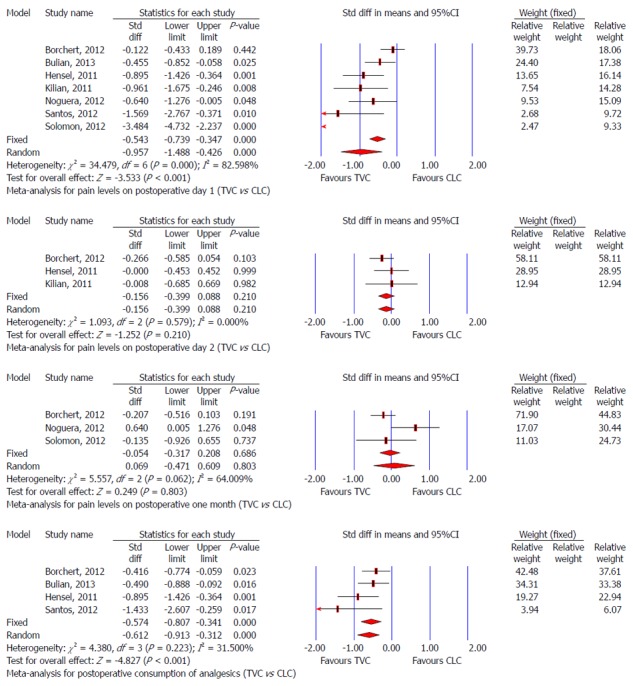
Results: There were 730 patients in nine controlled clinical trials. No significant difference was found regarding demographic characteristics (P > 0.5), including anesthetic risk score, age, body mass index, and abdominal surgical history between the TVC and CLC groups. Both groups had similar mortality, morbidity, and return to work after surgery. Patients in the TVC group had a lower pain score on postoperative day 1 (SMD: -0.957, 95%CI: -1.488 to -0.426, P < 0.001), needed less postoperative analgesic medication (SMD: -0.574, 95%CI: -0.807 to -0.341, P < 0.001) and stayed for a shorter time in hospital (MD: -1.004 d, 95%CI: -1.779 to 0.228, P = 0.011), but had longer operative time (MD: 17.307 min, 95%CI: 6.789 to 27.826, P = 0.001). TVC had no significant influence on postoperative sexual function and quality of life. Better cosmetic results and satisfaction were achieved in the TVC group.
Conclusion: TVC is safe and effective for gallbladder disease. However, vaginal injury might occur, and further trials are needed to compare TVC with CLC.
Keywords: Conventional laparoscopic cholecystectomy; Endoscopic surgery; Meta-analyses; Natural orifice; Transvaginal cholecystectomy.
Figures










Similar articles
-
Comparison of outcome and side effects between conventional and transvaginal laparoscopic cholecystectomy: a meta-analysis.Surg Laparosc Endosc Percutan Tech. 2014 Oct;24(5):395-9. doi: 10.1097/SLE.0000000000000066. Surg Laparosc Endosc Percutan Tech. 2014. PMID: 25084449
-
Systematic analysis of the safety and benefits of transvaginal hybrid-NOTES cholecystectomy.World J Gastroenterol. 2015 Oct 14;21(38):10915-25. doi: 10.3748/wjg.v21.i38.10915. World J Gastroenterol. 2015. PMID: 26478683 Free PMC article. Clinical Trial.
-
Postoperative pain after transvaginal cholecystectomy: single-center, double-blind, randomized controlled trial.Surg Endosc. 2014 Jun;28(6):1886-94. doi: 10.1007/s00464-013-3409-2. Epub 2014 Jan 24. Surg Endosc. 2014. PMID: 24464385 Clinical Trial.
-
Single-incision versus conventional laparoscopic cholecystectomy in patients with uncomplicated gallbladder disease: a meta-analysis.Surg Laparosc Endosc Percutan Tech. 2012 Dec;22(6):487-97. doi: 10.1097/SLE.0b013e3182685d0a. Surg Laparosc Endosc Percutan Tech. 2012. PMID: 23238374 Review.
-
Meta-analysis of single-port versus conventional laparoscopic cholecystectomy comparing body image and cosmesis.Br J Surg. 2017 Aug;104(9):1141-1159. doi: 10.1002/bjs.10574. Epub 2017 Jun 1. Br J Surg. 2017. PMID: 28569406 Review.
Cited by
-
Does obesity influence the results in Transvaginal Hybrid-NOTES cholecystectomy?Surg Endosc. 2018 Nov;32(11):4632-4638. doi: 10.1007/s00464-018-6216-y. Epub 2018 May 16. Surg Endosc. 2018. PMID: 29770882
-
Laparoscopic-Assisted Transvaginal Cholecystectomy - the US Military Experience With Long-Term Follow Up.JSLS. 2024 Jan-Mar;28(1):e2023.00059. doi: 10.4293/JSLS.2023.00059. JSLS. 2024. PMID: 38562949 Free PMC article.
-
[Implementation of hybrid-NOTES sigmoidectomy for diverticular disease : In a center for minimally invasive surgery].Chirurg. 2017 Jun;88(6):518-524. doi: 10.1007/s00104-016-0333-8. Chirurg. 2017. PMID: 27928602 German.
-
Single-Incision and Natural Orifice Translumenal Endoscopic Surgery in Switzerland.World J Surg. 2017 Feb;41(2):449-456. doi: 10.1007/s00268-016-3723-7. World J Surg. 2017. PMID: 27671014
-
Hybrid Transvaginal NOTES and Mini-Laparoscopic Colectomy: Benefit Through Synergy.JSLS. 2016 Oct-Dec;20(4):e2016.00062. doi: 10.4293/JSLS.2016.00062. JSLS. 2016. PMID: 27904307 Free PMC article.
References
-
- Bazzi WM, Stroup SP, Cohen SA, Sisul DM, Liss MA, Masterson JH, Kopp RP, Gudeman SR, Leeflang E, Palazzi KL, et al. Comparison of transrectal and transvaginal hybrid natural orifice transluminal endoscopic surgery partial nephrectomy in the porcine model. Urology. 2013;82:84–89. - PubMed
-
- Vieira JP, Linhares MM, Caetano EM, Moura RM, Asseituno V, Fuzyi R, Girão MJ, Ruano JM, Goldenberg A, de Jesus L Filho G, et al. Evaluation of the clinical and inflammatory responses in exclusively NOTES transvaginal cholecystectomy versus laparoscopic routes: an experimental study in swine. Surg Endosc. 2012;26:3232–3244. - PubMed
-
- Liu BR, Kong LJ, Song JT, Liu W, Yu H, Dou QF. Feasibility and safety of functional cholecystectomy by pure NOTES: a pilot animal study. J Laparoendosc Adv Surg Tech A. 2012;22:740–745. - PubMed
-
- Córdova H, Guarner-Argente C, Martínez-Pallí G, Navarro R, Rodríguez-D’Jesús A, Rodríguez de Miguel C, Beltrán M, Martínez-Zamora MÀ, Comas J, Lacy AM, et al. Gastric emptying is delayed in transgastric NOTES: a randomized study in swine. J Surg Res. 2012;174:e61–e67. - PubMed
-
- Bernhardt J, Köhler P, Rieber F, Diederich M, Schneider-Koriath S, Steffen H, Ludwig K, Lamadé W. Pure NOTES sigmoid resection in an animal survival model. Endoscopy. 2012;44:265–269. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
