

SR and LR Union Suture for the Treatment of Myopic Strabismus Fixus: Is Scleral Fixation Necessary?
- PMID: 25954751
- PMCID: PMC4410502
- DOI: 10.1155/2015/470473
SR and LR Union Suture for the Treatment of Myopic Strabismus Fixus: Is Scleral Fixation Necessary?
Abstract
Purpose: To evaluate and compare the effectiveness of scleral fixation SR and LR union suture and nonscleral fixation union suture for the treatment of myopic strabismus fixus.
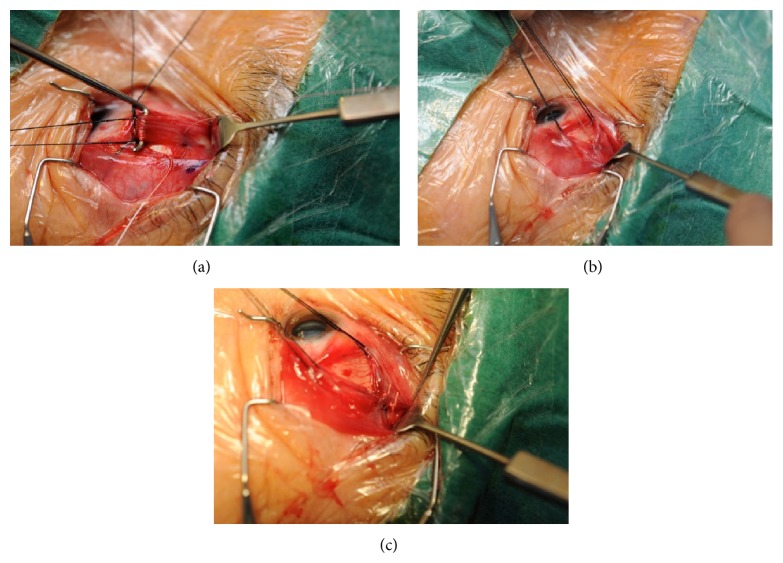
Methods: Retrospective review of 32 eyes of 22 patients with myopic strabismus fixus who had undergone union suture of superior rectus (SR) and lateral rectus (LR) with or without scleral fixation, and follow-up longer than 6 months at Hong Kong Eye Hospital from 2006 to 2013. Surgical techniques and outcomes in terms of ocular alignment are analyzed.
Results: There is significant overall improvement both in postoperative angle of esodeviation (P < 0.01) and postoperative range of movement (P = 0.042). Comparing between the sclera fixation group (11 eyes) versus nonscleral fixation group (21 eyes), the postoperative horizontal deviation, the postoperative vertical deviation, successful outcome, and the change in horizontal deviation were not significantly different (P > 0.05).
Conclusions: Union suture of SR and LR is an effective procedure in correcting myopic strabismus fixus. Fixation of the union suture to the sclera does not improve surgical outcome.
Figures

References
-
- Edwards M. H., Lam C. S. Y. The epidemiology of myopia in Hong Kong. Annals of the Academy of Medicine. 2004;33(1):34–38. - PubMed
-
- Tanaka A., Ohno-Matsui K., Shimada N., et al. Prevalence of strabismus in patients with pathologic myopia. Journal of Medical and Dental Sciences. 2010;57(1):75–82. - PubMed
-
- Aoki Y., Nishida Y., Hayashi O., et al. Magnetic resonance imaging measurements of extraocular muscle path shift and posterior eyeball prolapse from the muscle cone in acquired esotropia with high myopia. American Journal of Ophthalmology. 2003;136(3):482–489. doi: 10.1016/s0002-9394(03)00276-9. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
