

The safety and efficacy of antifibrinolytic therapy in neonatal cardiac surgery
- PMID: 25954976
- PMCID: PMC4425500
- DOI: 10.1371/journal.pone.0126514
The safety and efficacy of antifibrinolytic therapy in neonatal cardiac surgery
Abstract
Background: Neonates undergoing open-heart surgery are particularly at risk of postoperative bleeding requiring blood transfusion. Aprotinin has attained high efficacy in reducing the requirement for a blood transfusion following a cardiopulmonary bypass, but is seldom studied in the neonatal age group. The aim of this study was to compare the efficacy and adverse effects of aprotinin and tranexamic acid in neonates undergoing open-heart surgery at a single centre.
Methods: Between October 2003 and March 2008, perioperative data of 552 consecutive neonatal patients undergoing open-heart surgery in Children's Hospital Boston were reviewed. Among them, 177 did not receive antifibrinolytic therapy (Group A); 100 were treated with tranexamic acid only (Group B); and 275 patients received aprotinin with or without tranexamic acid (Group C). Except for antifibrinolytic therapy, the anaesthesiological and surgical protocols remained identical. Postoperative complications and in-hospital mortality were the primary study endpoints.
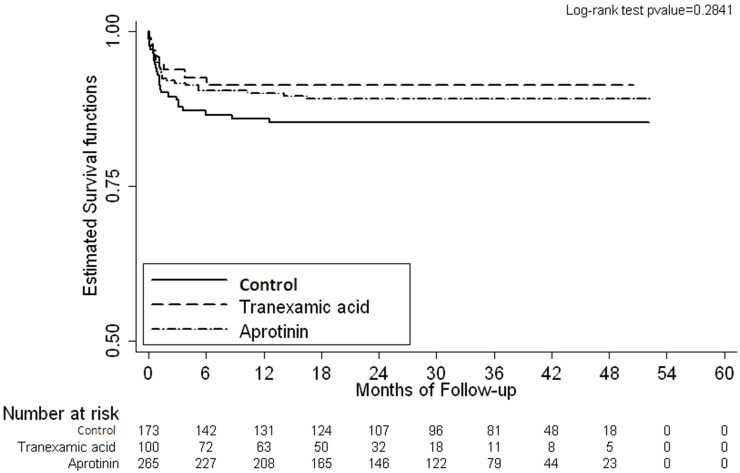
Results: Body weight and Risk Adjustment for Congenital Heart Surgery (RACHS-1) scores were statistically comparable among the three groups. No statistically significant differences were observed between the duration of hospitalization, chest tube drainage, reexploration for bleeding, and kidney function impairment. In Group C, less blood was transfused within 24 hours than in GroupB. Operative mortality was similar among the three groups.
Conclusion: No further risk and kidney injury were observed in the use of aprotinin in neonatal cardiac surgery, aprotinin demonstrated a reduced requirement for blood transfusion compared with tranexamic acid. Our data provide reasonable evidence that aprotinin and tranexamic acid are safe and efficacious as antifibrinolytic modalities in neonatal patients undergoing cardiac surgery.
Conflict of interest statement
References
-
- Levy JH, Tanaka KA. Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg 2003;75:S715–S720. - PubMed
-
- Paparella D, Brister SJ, Buchanan MR. Coagulation disorders of cardiopulmonary bypass: a review. Intensive Care Med 2004;30:1873–1881. - PubMed
-
- Shen I, Giacomuzzi C, Ungerleider RM. Current strategies for optimizing the use of cardiopulmonary bypass in neonates and infants. Ann Thorac Surg 2003;75:S729–S734. - PubMed
-
- Kern FH, Morana NJ, Sears JJ, Hickey PR. Coagulation defects in neonates during cardiopulmonary bypass. Ann Thorac Surg 1992;54:541–546. - PubMed
-
- Mossinger H, Dietrich W, Braun SL, Jochum M, Meisner H, Richter JA. High-dose aprotinin reduces activation of hemostasis, allogeneic blood requirement, and duration of postoperative ventilation in pediatric cardiac surgery. Ann Thorac Surg 2003;75:430–437. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
