

Impact of Smoking and Brain Metastasis on Outcomes of Advanced EGFR Mutation Lung Adenocarcinoma Patients Treated with First Line Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors
- PMID: 25955322
- PMCID: PMC4425557
- DOI: 10.1371/journal.pone.0123587
Impact of Smoking and Brain Metastasis on Outcomes of Advanced EGFR Mutation Lung Adenocarcinoma Patients Treated with First Line Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors
Abstract
Objectives: This purpose of this study was to examine clinical-pathologic factors--particularly smoking and brain metastases--in EGFR mutation positive (M(+)) lung adenocarcinoma (ADC) to determine their impact on survival in patients treated with first line EGFR TKI.
Methods: A retrospective review of EGFR mutation reflex testing experience for all ADC diagnosed at a tertiary Asian cancer centre from January 2009 to April 2013. Amongst this cohort, patients with advanced EGFR M(+) ADC treated with first line EGFR TKI were identified to determine factors that influence progression free and overall survival.
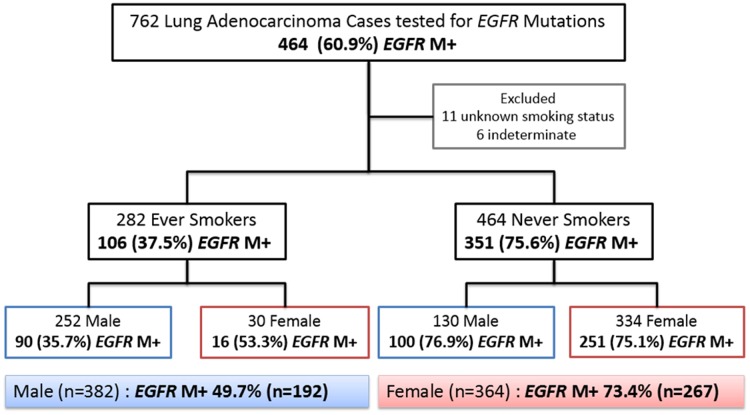
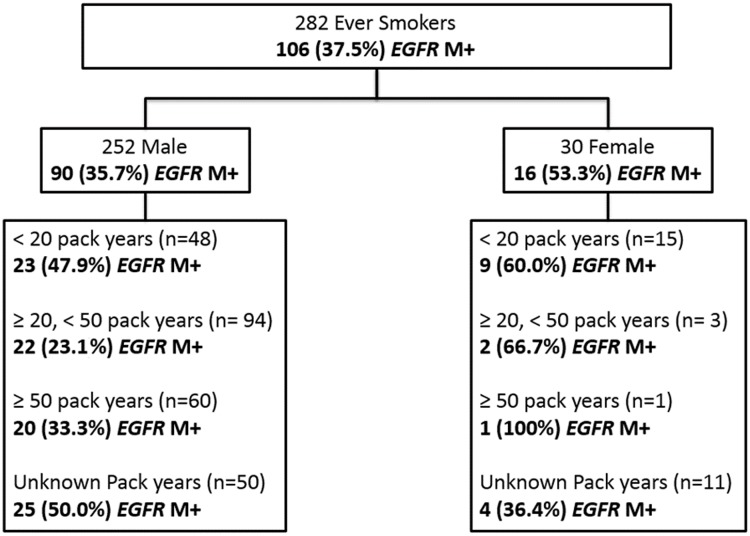
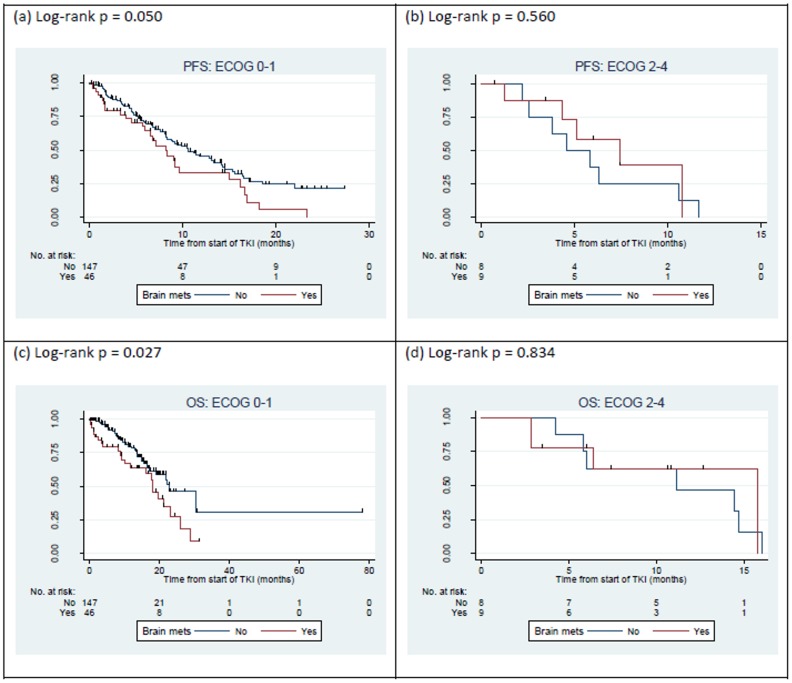
Results: 444/742 (59.8%) ADC reflex tested for EGFR mutations were EGFR M(+.) Amongst never-smokers (n=468), EGFR M(+) were found in 74.5% of females and 76.3% of males, and amongst ever smokers (n=283), in 53.3% of females and 35.6% of males. Exon 20 mutations were found more commonly amongst heavy smokers (> 50 pack years and > 20 pack years, Pearson's chi square p=0.044, and p=0.038 respectively). 211 patients treated with palliative first line TKI had a median PFS and OS of 9.2 and 19.6 months respectively. 26% of patients had brain metastasis at diagnosis. This was significantly detrimental to overall survival (HR 1.85, CI 1.09-3.16, p=0.024) on multivariate analysis. There was no evidence that smoking status had a significant impact on survival.
Conclusions: The high prevalence of EGFR M(+) in our patient population warrants reflex testing regardless of gender and smoking status. Smoking status and dosage did not impact progression free or overall survival in patients treated with first line EGFR TKI. The presence of brain metastasis at diagnosis negatively impacts overall survival.
Conflict of interest statement
Figures

References
-
- Fukuoka M, Wu Y-L, Thongprasert S, Sunpaweravong P, Leong S-S, Sriuranpong V, et al. Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). Journal of Clinical Oncology. 2011. July 20;29(21):2866–74. 10.1200/JCO.2010.33.4235 - DOI - PubMed
-
- Zhou C, Wu Y-L, Chen G, Feng J, Liu X-Q, Wang C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011. August;12(8):735–42. 10.1016/S1470-2045(11)70184-X - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
