

Trends in Tracheostomy for Mechanically Ventilated Patients in the United States, 1993-2012
- PMID: 25955332
- PMCID: PMC4595669
- DOI: 10.1164/rccm.201502-0239OC
Trends in Tracheostomy for Mechanically Ventilated Patients in the United States, 1993-2012
Abstract
Rationale: National trends in tracheostomy for mechanical ventilation (MV) patients are not well characterized.
Objectives: To investigate trends in tracheostomy use, timing, and outcomes in the United States.
Methods: We calculated estimates of tracheostomy use and outcomes from the National Inpatient Sample from 1993 to 2012. We used hierarchical models to determine factors associated with tracheostomy use among MV patients.
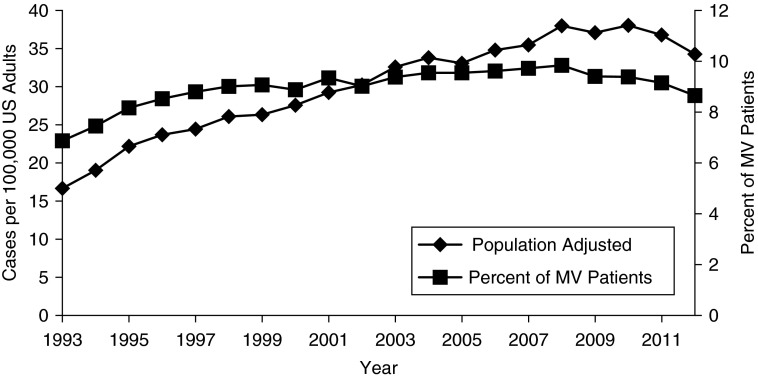
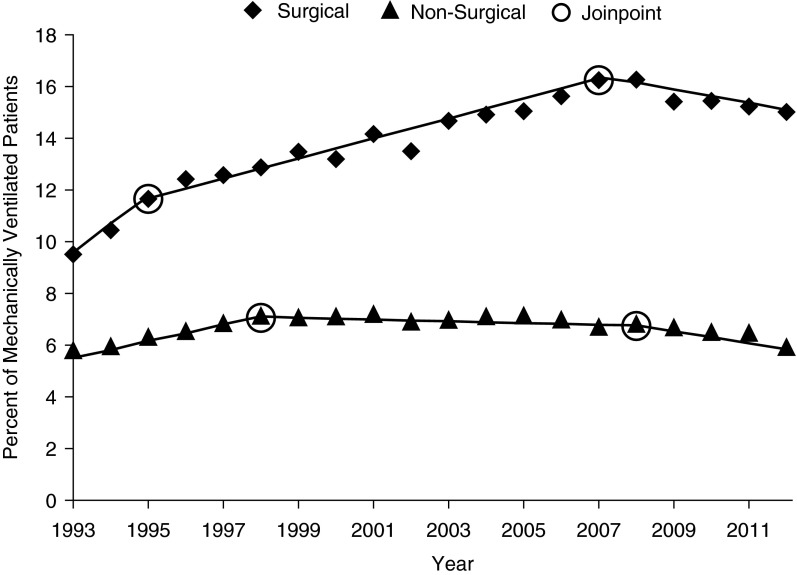
Measurements and main results: We identified 1,352,432 adults who received tracheostomy from 1993 to 2012 (9.1% of MV patients). Tracheostomy was more common in surgical patients, men, and racial/ethnic minorities. Age-adjusted incidence of tracheostomy increased by 106%, rising disproportionately to MV use. Among MV patients, tracheostomy rose from 6.9% in 1993 to 9.8% in 2008, and then it declined to 8.7% in 2012 (P < 0.0001). Increases in tracheostomy use were driven by surgical patients (9.5% in 1993; 15.0% in 2012; P < 0.0001), with little change among nonsurgical patients (5.8% in 1993; 5.9% in 2012; P < 0.0001). Over time, tracheostomies were performed earlier (median, 11 d in 1998; 10 d in 2012; P < 0.0001), whereas hospital length of stay declined (median, 39 d in 1993; 26 d in 2012; P < 0.0001), discharges to long-term facilities increased (40.1% vs. 71.9%; P < 0.0001), and hospital mortality declined (38.1% vs. 14.7%; P < 0.0001).
Conclusions: Over the past two decades, tracheostomy use rose substantially in the United States until 2008, when use began to decline. The observed dramatic increase in discharge of tracheostomy patients to long-term care facilities may have significant implications for clinical care, healthcare costs, policy, and research. Future studies should include long-term facilities when analyzing outcomes of tracheostomy.
Keywords: United States; epidemiology; mechanical ventilation; tracheostomy.
Figures
Comment in
-
The Implications of a Tracheostomy for Discharge Destination.Am J Respir Crit Care Med. 2015 Aug 15;192(4):404-5. doi: 10.1164/rccm.201505-1007ED. Am J Respir Crit Care Med. 2015. PMID: 26278790 No abstract available.
References
-
- Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. 2010;38:1947–1953. - PubMed
-
- Lam S, Ridley S. Critically ill medical patients, their demographics and outcome. Anaesthesia. 1999;54:845–852. - PubMed
-
- Needham DM, Bronskill SE, Calinawan JR, Sibbald WJ, Pronovost PJ, Laupacis A. Projected incidence of mechanical ventilation in Ontario to 2026: preparing for the aging baby boomers. Crit Care Med. 2005;33:574–579. - PubMed
-
- Carson SS, Bach PB. The epidemiology and costs of chronic critical illness. Crit Care Clin. 2002;18:461–476. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
