

Comparative and cost effectiveness of telemedicine versus telephone counseling for smoking cessation
- PMID: 25956257
- PMCID: PMC4468596
- DOI: 10.2196/jmir.3975
Comparative and cost effectiveness of telemedicine versus telephone counseling for smoking cessation
Erratum in
-
Metadata Correction: Comparative and Cost Effectiveness of Telemedicine Versus Telephone Counseling for Smoking Cessation.J Med Internet Res. 2015 Jun 15;17(6):e124. doi: 10.2196/jmir.4642. J Med Internet Res. 2015. PMID: 26075409 Free PMC article. No abstract available.
Abstract
Background: In rural America, cigarette smoking is prevalent and health care providers lack the time and resources to help smokers quit. Telephone quitlines are important avenues for cessation services in rural areas, but they are poorly integrated with local health care resources.
Objective: The intent of the study was to assess the comparative effectiveness and cost effectiveness of two models for delivering expert tobacco treatment at a distance: telemedicine counseling that was integrated into smokers' primary care clinics (Integrated Telemedicine-ITM) versus telephone counseling, similar to telephone quitline counseling, delivered to smokers in their homes (Phone).
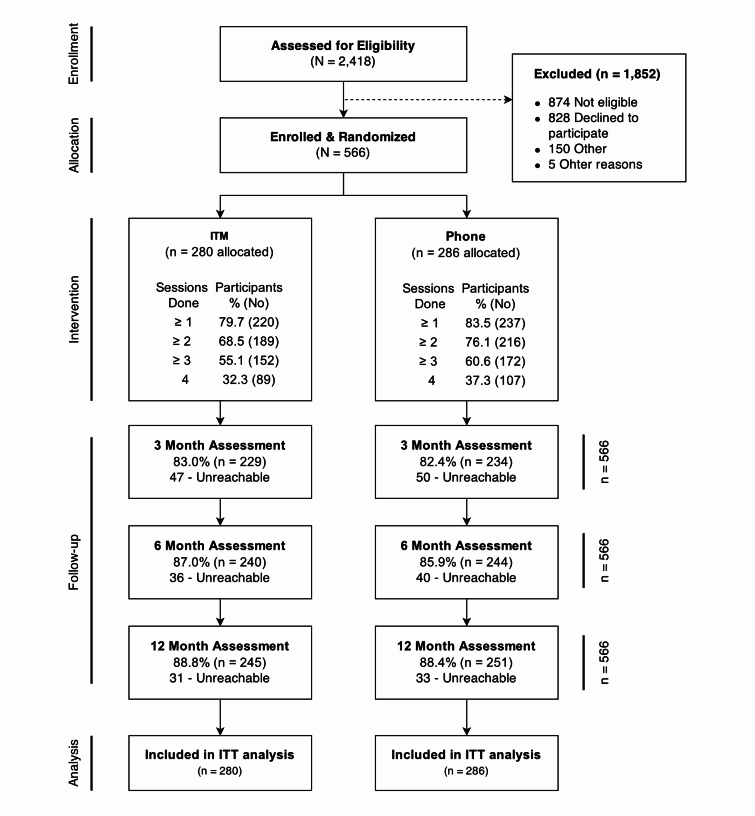
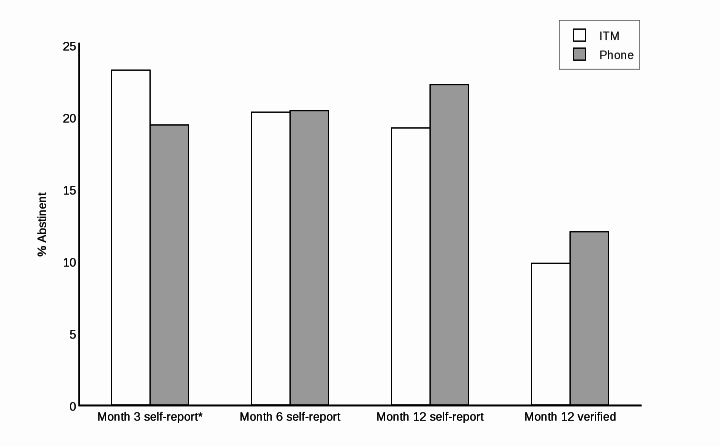
Methods: Smokers (n=566) were recruited offline from 20 primary care and safety net clinics across Kansas. They were randomly assigned to receive 4 sessions of ITM or 4 sessions of Phone counseling. Patients in ITM received real-time video counseling, similar to Skype, delivered by computer/webcams in clinic exam rooms. Three full-time equivalent trained counselors delivered the counseling. The counseling duration and content was the same in both groups and was available in Spanish or English. Both groups also received identical materials and assistance in selecting and obtaining cessation medications. The primary outcome was verified 7-day point prevalence smoking abstinence at month 12, using an intent-to-treat analysis.
Results: There were no significant baseline differences between groups, and the trial achieved 88% follow-up at 12 months. Verified abstinence at 12 months did not significantly differ between ITM or Phone (9.8%, 27/280 vs 12%, 34/286; P=.406). Phone participants completed somewhat more counseling sessions than ITM (mean 2.6, SD 1.5 vs mean 2.4, SD 1.5; P=.0837); however, participants in ITM were significantly more likely to use cessation medications than participants in Phone (55.9%, 128/280 vs 46.1%, 107/286; P=.03). Compared to Phone participants, ITM participants were significantly more likely to recommend the program to a family member or friend (P=.0075). From the combined provider plus participant (societal) perspective, Phone was significantly less costly than ITM. Participants in ITM had to incur time and mileage costs to travel to clinics for ITM sessions. From the provider perspective, counseling costs were similar between ITM (US $45.46, SD 31.50) and Phone (US $49.58, SD 33.35); however, total provider costs varied widely depending on how the clinic space for delivering ITM was valued.
Conclusions: Findings did not support the superiority of ITM over telephone counseling for helping rural patients quit smoking. ITM increased utilization of cessation pharmacotherapy and produced higher participant satisfaction, but Phone counseling was significantly less expensive. Future interventions could combine elements of both approaches to optimize pharmacotherapy utilization, counseling adherence, and satisfaction. Such an approach could commence with a telemedicine-delivered clinic office visit for pharmacotherapy guidance, and continue with telephone or real-time video counseling delivered via mobile phones to flexibly deliver behavioral support to patients where they most need it-in their homes and communities.
Trial registration: Clinicaltrials.gov NCT00843505; http://clinicaltrials.gov/ct2/show/NCT00843505 (Archived by WebCite at http://www.webcitation.org/6YKSinVZ9).
Keywords: Internet; primary care; rural; smoking cessation, RCT; telemedicine.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- World Health Organization . WHO Report on the Global Tobacco Epidemic: The MPOWER package. Geneva: World Health Organization; 2008. [2015-02-21]. http://www.who.int/tobacco/mpower/en/
-
- Pleis JR, Lucas JW, Ward BW. National Center for Health Statistics. 2009. [2015-05-05]. Summary health statistics for U.S. adults: National Health Interview Survey, 2008 http://www.cdc.gov/nchs/data/series/sr_10/sr10_242.pdf. - PubMed
-
- Fiore MC, Jaen CR, Baker TB. Clinical Practice Guideline. Rockville, MD: Department of Health and Human Services. Public Health Service; 2008. [2015-05-05]. Treating Tobacco Use and Dependence: 2008 Update http://www.ahrq.gov/professionals/clinicians-providers/guidelines-recomm....
-
- Robinson M D, Laurent S L, Little J M. Including smoking status as a new vital sign: it works! J Fam Pract. 1995 Jun;40(6):556–61. - PubMed
-
- Centers for Disease ControlPrevention (CDC) Physician and other health-care professional counseling of smokers to quit--United States, 1991. MMWR Morb Mortal Wkly Rep. 1993 Nov 12;42(44):854–7. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
