

Antifibrinolytic drugs for acute traumatic injury
- PMID: 25956410
- PMCID: PMC10589907
- DOI: 10.1002/14651858.CD004896.pub4
Antifibrinolytic drugs for acute traumatic injury
Abstract
Background: Uncontrolled bleeding is an important cause of death in trauma victims. Antifibrinolytic treatment has been shown to reduce blood loss following surgery and may also be effective in reducing blood loss following trauma.
Objectives: To assess the effect of antifibrinolytic drugs in patients with acute traumatic injury.
Search methods: We ran the most recent search in January 2015. We searched the Cochrane Injuries Group's Specialised Register, The Cochrane Library, Ovid MEDLINE(R), Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily and Ovid OLDMEDLINE(R), Embase Classic+Embase (OvidSP), PubMed and clinical trials registries.
Selection criteria: Randomised controlled trials of antifibrinolytic agents (aprotinin, tranexamic acid [TXA], epsilon-aminocaproic acid and aminomethylbenzoic acid) following acute traumatic injury.
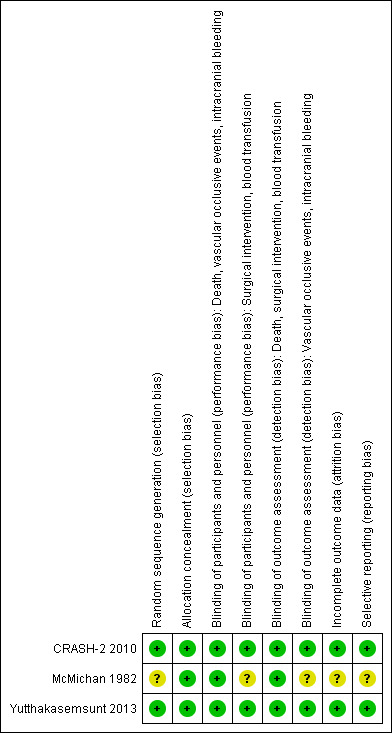
Data collection and analysis: From the results of the screened electronic searches, bibliographic searches, and contacts with experts, two authors independently selected trials meeting the inclusion criteria, and extracted data. One review author assessed the risk of bias for key domains.Outcome measures included: mortality at end of follow-up (all-cause); adverse events (specifically vascular occlusive events [myocardial infarction, stroke, deep vein thrombosis or pulmonary embolism] and renal failure); number of patients undergoing surgical intervention or receiving blood transfusion; volume of blood transfused; volume of intracranial bleeding; brain ischaemic lesions; death or disability.We rated the quality of the evidence as 'high', 'moderate', 'low' or 'very low' according to the GRADE approach.
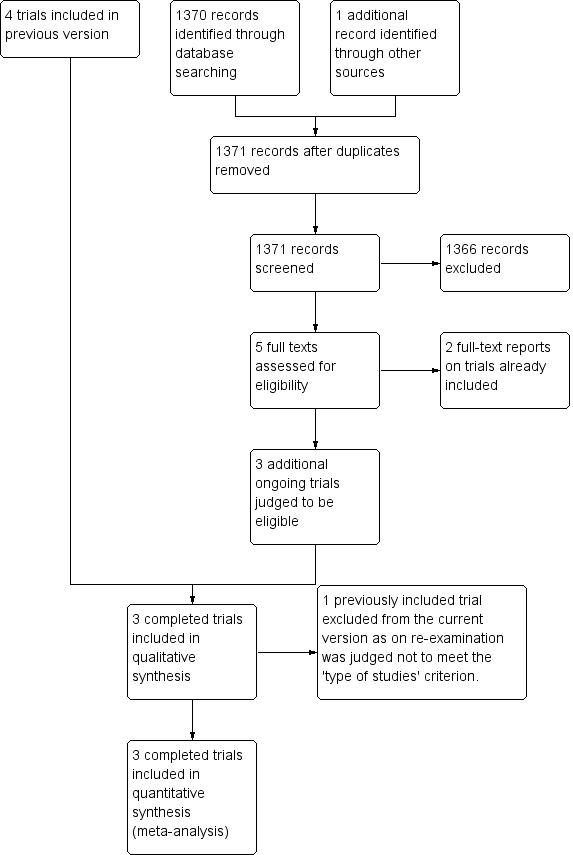
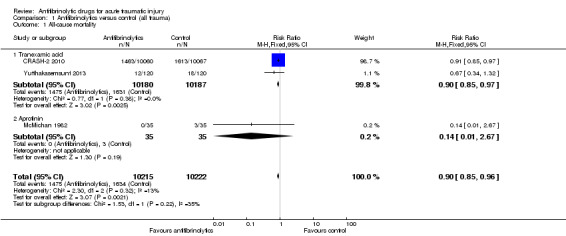
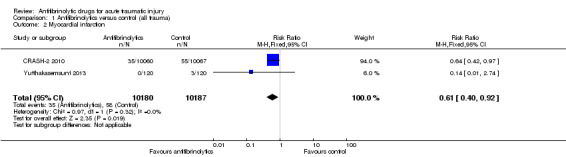
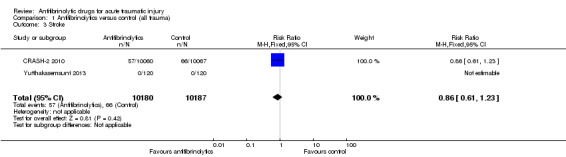
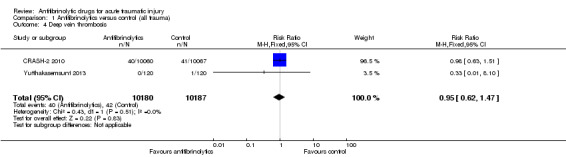
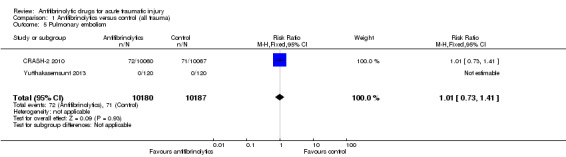
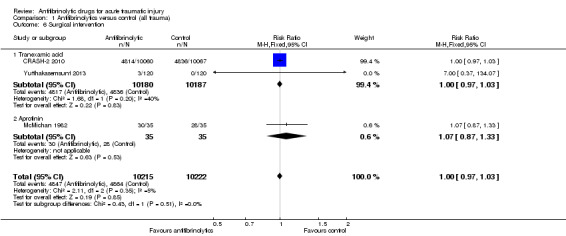
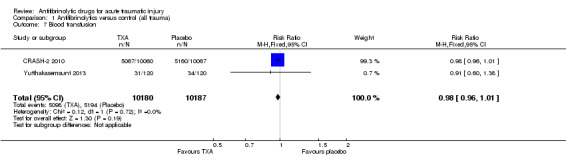
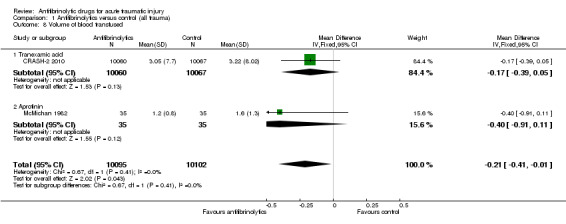
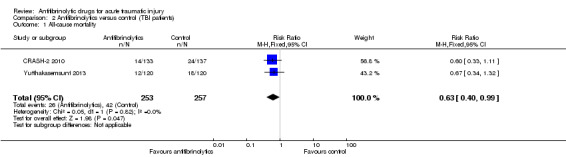
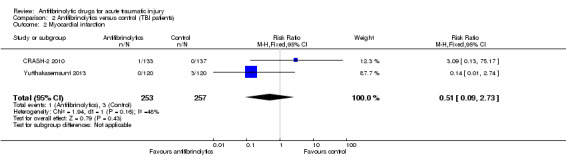
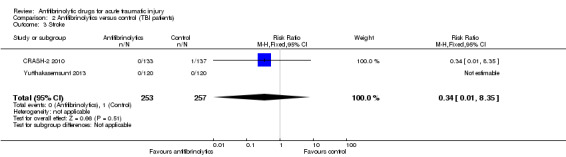
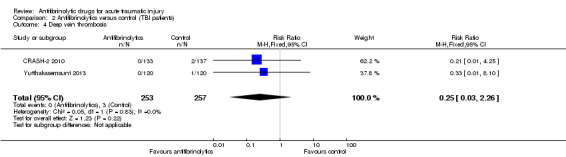
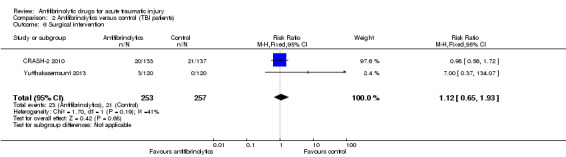
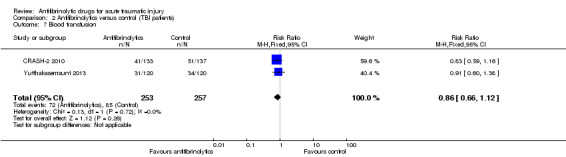
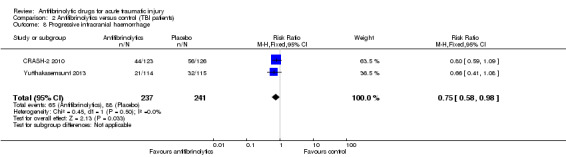
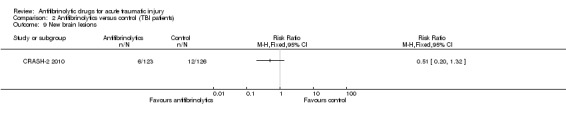
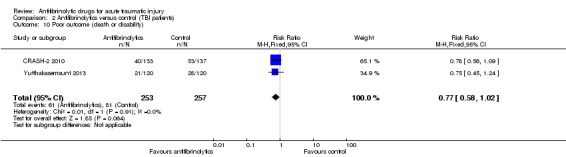
Main results: Three trials met the inclusion criteria.Two trials (n = 20,451) assessed the effect of TXA. The larger of these (CRASH-2, n = 20,211) was conducted in 40 countries and included patients with a variety of types of trauma; the other (n = 240) restricted itself to those with traumatic brain injury (TBI) only.One trial (n = 77) assessed aprotinin in participants with major bony trauma and shock.The pooled data show that antifibrinolytic drugs reduce the risk of death from any cause by 10% (RR 0.90, 95% CI 0.85 to 0.96; P = 0.002) (quality of evidence: high). This estimate is based primarily on data from the CRASH-2 trial of TXA, which contributed 99% of the data.There is no evidence that antifibrinolytics have an effect on the risk of vascular occlusive events (quality of evidence: moderate), need for surgical intervention or receipt of blood transfusion (quality of evidence: high). There is no evidence for a difference in the effect by type of antifibrinolytic (TXA versus aprotinin) however, as the pooled analyses were based predominantly on trial data concerning the effects of TXA, the results can only be confidently applied to the effects of TXA. The effects of aprotinin in this patient group remain uncertain.There is some evidence from pooling data from one study (n = 240) and a subset of data from CRASH-2 (n = 270) in patients with TBI which suggest that TXA may reduce mortality although the estimates are imprecise, the quality of evidence is low, and uncertainty remains. Stronger evidence exists for the possibility of TXA reducing intracranial bleeding in this population.
Authors' conclusions: TXA safely reduces mortality in trauma patients with bleeding without increasing the risk of adverse events. TXA should be given as early as possible and within three hours of injury, as further analysis of the CRASH-2 trial showed that treatment later than this is unlikely to be effective and may be harmful. Although there is some promising evidence for the effect of TXA in patients with TBI, substantial uncertainty remains.Two ongoing trials being conducted in patients with isolated TBI should resolve these remaining uncertainties.
Conflict of interest statement
KK works at the LSHTM Clinical Trials Unit to support its programme of ongoing trials into the effects of tranexamic acid in clinically important haemorrhage, including the WOMAN trial of tranexamic acid for the treatment of postpartum haemorrhage, the CRASH‐3 trial of tranexamic acid for the treatment of traumatic brain injury and the HALT‐IT trial of tranexamic acid for the treatment of gastrointestinal bleeding.
IR is chief investigator of the ongoing WOMAN trial of tranexamic acid for the treatment of postpartum haemorrhage, the CRASH‐3 trial of tranexamic acid for the treatment of traumatic brain injury and the HALT‐IT trial of tranexamic acid for the treatment of gastrointestinal bleeding. IR was also chief investigator of the CRASH‐2 trial that is included in this review. LSHTM has received funds from pharmaceutical companies to pay for the drug and placebo used in these randomised controlled trials of tranexamic acid in acute severe bleeding. These funds are declared in the relevant publications. IR also provided advice on the protocol of the trial by Yutthakasemsunt 2013 and commented on the final manuscript.
HS is an investigator and grant holder for the WOMAN trial of tranexamic acid for the treatment of postpartum haemorrhage, the CRASH‐3 trial of tranexamic acid for the treatment of traumatic brain injury and the HALT‐IT trial of tranexamic acid for the treatment of gastrointestinal bleeding. HS was also an investigator in the CRASH‐2 trial that is included in this review.
TC is an investigator in the ongoing CRASH‐3 and HALT‐IT trials and was also an investigator in the CRASH‐2 trial that is included in this review.
Figures
Update of
-
Antifibrinolytic drugs for acute traumatic injury.Cochrane Database Syst Rev. 2012;12:CD004896. doi: 10.1002/14651858.CD004896.pub3. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2015 May 09;(5):CD004896. doi: 10.1002/14651858.CD004896.pub4. PMID: 23418644 Updated.
References
References to studies included in this review
CRASH‐2 2010 {published and unpublished data}
-
- CRASH‐2 trial collaborators, Roberts I, Shakur H, Afolabi A, Brohi K, Coats T, et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH‐2 randomised controlled trial. Lancet 2011;377(9771):1096‐101. - PubMed
-
- CRASH‐2 trial collaborators, Shakur H, Roberts I, Bautista R, Caballero J, Coats T, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH‐2): a randomised, placebo‐controlled trial. Lancet 2010;376:23‐32. - PubMed
McMichan 1982 {published data only}
-
- McMichan JC, Rosengarten DS, McNeur JC, Philipp E. Posttraumatic lung syndrome. Definition, diagnosis, and therapy [Das Posttraumatische Lungen‐Syndrom Defintion, Diagnose und Therapie]. Medizinische Welt 1976;76(48):2331‐9. - PubMed
-
- McMichan JC, Rosengarten DS, McNeur JC, Philipp E. Pulmonary failure after major trauma and shock. Intensive Care Medicine 1977;3:Abstract no. 37.
-
- McMichan JC, Rosengarten DS, Philipp E. Prophylaxis of post‐traumatic pulmonary insufficiency by protease‐inhibitor therapy with aprotinin: a clinical study. Circulatory Shock 1982;9(2):107‐16. - PubMed
-
- Rosengarten DS, McMichan JC, McNeur JC, Philipp E. Platelet and pulmonary insufficiency after bony trauma. Intensive Care Medicine 1977;3:Abstract no. 327.
-
- Rosengarten DS, McMichan JC, Philipp E. The effect of prophylactic proteinase inhibitor therapy on post‐traumatic pulmonary insufficiency and platelet counts. Advances in Experimental Medicine and Biology 1979;120B:349‐60. - PubMed
Yutthakasemsunt 2013 {published and unpublished data}
-
- Yutthakasemsunt S, Kittiwattanagul W, Piyavechvirat P, Thinkhamrop B, Phuenpathom N, Lumbiganon P. Tranexamic Acid for preventing progressive intracranial hemorrhage in adults with traumatic brain injury; a preliminary report. National Neurotrauma Symposium. 14‐17 July 2010.
References to studies excluded from this review
Auer 1979 {published data only}
-
- Auer LM, Marth E, Heppner F, Holasek A. Proteolytic enzyme activity in patients with severe head injury and the effect of a proteinase inhibitor. Acta Neurochirurgica 1979;49(3‐4):207‐17. - PubMed
Gierhake 1971 {published data only}
-
- Gierhake FW, Grabow L, Spitzer G, Muller C, Braun R, Hessler C, et al. Protease inhibitors and wound healing. Results of a double blind study. Der Chirurg 1979;42(8):360‐3. - PubMed
Husted 2003 {published data only}
-
- Husted H, Blond L, Sonne‐Holm S, Holm G, Jacobsen TW, Gebuhr P. Tranexamic acid reduces blood loss and blood transfusions in primary hip arthroplasty: a prospective randomized double blind study in 40 patients. Acta Orthopaedica Scandinavica 2003;74(6):665‐9. - PubMed
Klobow 1977a {published data only}
-
- Klobow H, Barthels M, Oestern HJ, Sturm J, Wannske M, Schaps D. Early changes of the coagulation system in multiple injuries and their modification with heparin and Trasyolol. Chirurgisches Forum für experimentelle und klinishe Forschung 1977;April:119‐23. - PubMed
Klobow 1977b {published data only}
-
- Klobow H, Barthels M, Oestern HJ, Sturm J, Trentz O, Wannske M. Early changes in the coagulation and fibrinolytic system in patients receiving heparin or trasylol after massive trauma. Intensive Care Medicine 1977;3:Abstract no 324.
Kuiian 1999 {published data only}
-
- Kuiian SM, Pogosov VS, Kokliaeva NV, Tiukov VL, Riazanov VB, Gur'ianov VA, et al. The use of tranexamic acid as an anesthetic component in ENT surgeries in patients with high surgical‐anesthetic risk and in hemorrhagic shock intensive therapy. Vestnik Otorinolaringologii 1999;1:47‐51. - PubMed
Loew 1970 {published data only}
-
- Loew D. Pathophysiologic importance of kinins in traumatic shock. Langenbecks Archiv für Chirurgie 1970;327:1042‐6. - PubMed
Nissen 1989 {published data only}
-
- Nissen R, Loeschke S, Peters A. Pharmacological treatment of post‐traumatic oedema to allow early functional exercise. Langenbecks Archiv für Chirurgie 1989;Supplement II:475‐8. - PubMed
Schneider 1976 {published data only}
-
- Schneider B. Results of a field study on the therapeutic value of aprotinin in traumatic shock. Arzneimittel Forshung 1976;26:1606‐10. - PubMed
References to ongoing studies
NCT01402882 {published data only}
-
- Dewan Y, Komolafe EO, Mejía‐Mantilla JH, Perel P, Roberts I, Shakur H, on behalf CRASH‐3 Collaborators. CRASH‐3 ‐ tranexamic acid for the treatment of significant traumatic brain injury: study protocol for an international randomized, double‐blind, placebo‐controlled trial. Trials 2012;13:87. - PMC - PubMed
-
- NCT01402882. Tranexamic acid for the treatment of significant traumatic brain injury: an international randomised, double blind placebo controlled trial. http://clinicaltrials.gov/ct2/show/NCT01402882.
NCT01990768 {published data only}
-
- NCT01990768. Prehospital tranexamic acid use for traumatic brain injury (TXA). http://clinicaltrials.gov/ct2/show/NCT01990768.
NCT02086500 {published data only}
-
- NCT02086500. Study of tranexamic acid during air medical prehospital transport trial (STAAMP Trial). https://clinicaltrials.gov/ct2/show/NCT02086500. - PMC - PubMed
NCT02187120 {published data only}
-
- NCT02187120. Pre‐hospital anti‐fibrinolytics for traumatic coagulopathy and haemorrhage (the PATCH study). https://clinicaltrials.gov/show/NCT02187120.
Additional references
BTF 2000
-
- The Brain Trauma Foundation. The American Association of Neurological Surgeons. The Joint Section on Neurotrauma and Critical Care. Hypotension. Journal of Neurotrauma 2000;17(6‐7):591‐5. - PubMed
CRASH‐2 2011
-
- CRASH‐2 collaborators, Roberts I, Shakur H, Afolabi A, Brohi K, Coats T, et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH‐2 randomised controlled trial. Lancet 2011;377(9771):1096‐101. - PubMed
GBD 2013
GRADEpro 2014 [Computer program]
-
- McMaster University. GRADEpro. Hamilton, Ontario: McMaster University, 2014.
Guerriero 2011
Henry 2011
Heymann 1992
-
- Heymann SJ, Brewer TF. The problem of transfusion associated acquired immunodeficiency syndrome in Africa: a quantitative approach. American Journal of Infection Control 1992;20:256‐62. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration 2011. The Cochrane Collaboration. Available from www.cochrane‐handbook.org.
Ker 2012
-
- Ker K, Kiriya J, Perel P, Edwards P, Shakur H, Roberts I. Avoidable mortality from giving tranexamic acid to bleeding trauma patients: an estimation based on WHO mortality data, a systematic literature review and data from the CRASH‐2 trial. BMC Emergency Medicine 2012;12(3):doi:10.1186/1471‐227X‐12‐3. - PMC - PubMed
Kiwanuka 2004
-
- Kiwanuka N, Gray RH, Serwadda D, Li X, Sewankambo NK, Kigozi G, et al. The incidence of HIV‐1 associated with injections and transfusions in a prospective cohort, Raki, Uganda. AIDS 2004;18:343‐3. - PubMed
Lawson 2004
-
- Lawson JH, Murphy MP. Challenges for providing effective hemostasis in surgery and trauma. Seminars in Hematology 2004;41(1 Suppl 1):55‐64. - PubMed
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Perel 2010
Sander 2002
-
- Sander A. The Extended Glasgow Outcome Scale. The Center for Outcome Measurement in Brain Injury.http://www.tbims.org/combi/gose (accessed April 12, 2015) 2002.
Sauaia 1995
-
- Sauaia A, Moore FA, Moore E, Moser K, Brennan R, Read RA, et al. Epidemiology of trauma deaths: a reassessment. Journal of Trauma 1995;38:185‐93. - PubMed
Teasdale 1974
-
- Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2:81‐4. - PubMed
Teasdale 1979
-
- Teasdale G, Murray G, Parker L, Jennett B. Adding up the Glasgow Coma Score. Acta Neurochirugica 1979;28(Supplement):13‐6. - PubMed
References to other published versions of this review
Coats 2004
Roberts 2004
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous