

Proteinase 3-ANCA Vasculitis versus Myeloperoxidase-ANCA Vasculitis
- PMID: 25956510
- PMCID: PMC4587702
- DOI: 10.1681/ASN.2014090903
Proteinase 3-ANCA Vasculitis versus Myeloperoxidase-ANCA Vasculitis
Abstract
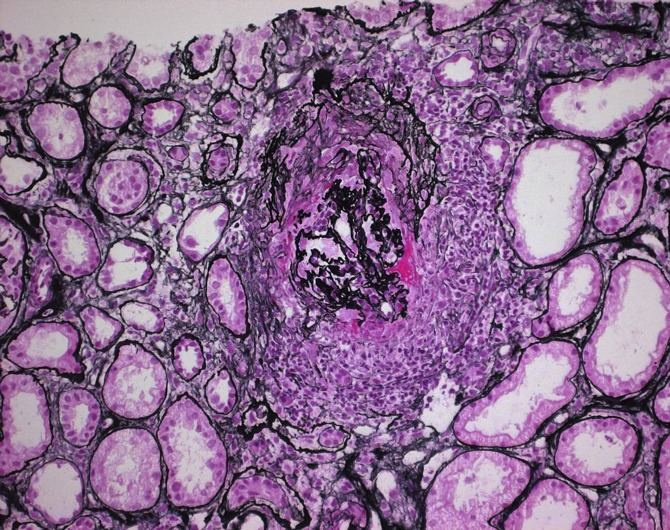
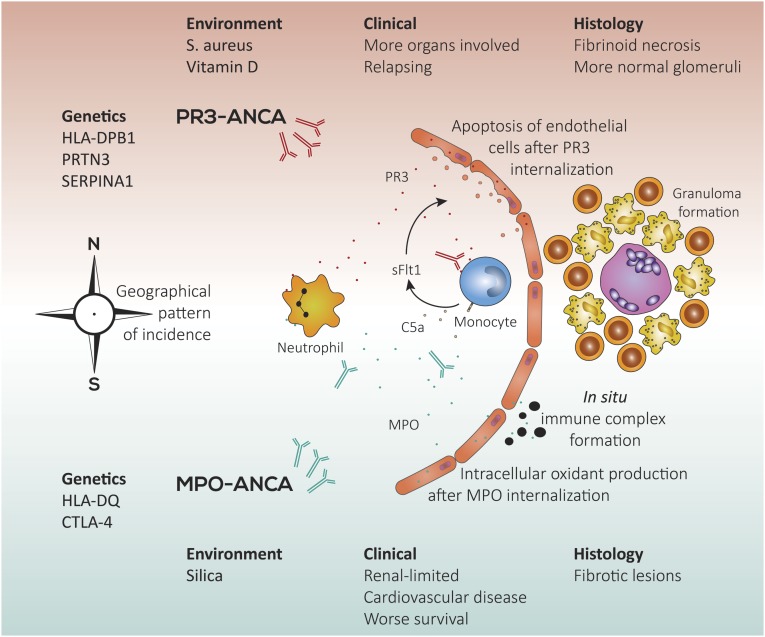
In patients with GN or vasculitis, ANCAs are directed against proteinase 3 (PR3) or myeloperoxidase (MPO). The differences between PR3-ANCA-associated vasculitis (AAV) and MPO-AAV described in the past have been supplemented during the last decade. In this review, we discuss the differences between these two small-vessel vasculitides, focusing especially on possible etiologic and pathophysiologic differences. PR3-AAV is more common in northern parts of the world, whereas MPO-AAV is more common in southern regions of Europe, Asia, and the Pacific, with the exception of New Zealand and Australia. A genetic contribution has been extensively studied, and there is a high prevalence of the HLA-DPB1*04:01 allele in patients with PR3-AAV as opposed to patients with MPO-AAV and/or healthy controls. Histologically, MPO-AAV and PR3-AAV are similar but show qualitative differences when analyzed carefully. Clinically, both serotypes are difficult to distinguish, but quantitative differences are present. More organs are affected in PR3-AAV, whereas renal limited vasculitis occurs more often in patients with MPO-AAV. For future clinical trials, we advocate classifying patients by ANCA serotype as opposed to the traditional disease type classification.
Keywords: ANCA; glomerulonephritis; vasculitis.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Cohen Tervaert JW, Damoiseaux J. Fifty years of antineutrophil cytoplasmic antibodies (ANCA) testing: do we need to revise the international consensus statement on testing and reporting on ANCA? APMIS Suppl 127: 55–59, 2009 - PubMed
-
- van der Woude FJ, Rasmussen N, Lobatto S, Wiik A, Permin H, van Es LA, van der Giessen M, van der Hem GK, The TH: Autoantibodies against neutrophils and monocytes: tool for diagnosis and marker of disease activity in Wegener’s granulomatosis. Lancet 1: 425–429, 1985 - PubMed
-
- Klinger H: Grenzformen der Periarteriitis nodosa. Frankf Z Pathol 42: 455–480, 1931
-
- Wegener F: Über eine eigenartige rhinogene Granulomatose mit besonderer Beteiligung des Arteriensystems und der Nieren. Beitr Pathol Anat 102: 36–68, 1939
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
