

Vapoenucleation of the prostate using a high-power thulium laser: a one-year follow-up study
- PMID: 25956819
- PMCID: PMC4438483
- DOI: 10.1186/s12894-015-0032-7
Vapoenucleation of the prostate using a high-power thulium laser: a one-year follow-up study
Abstract
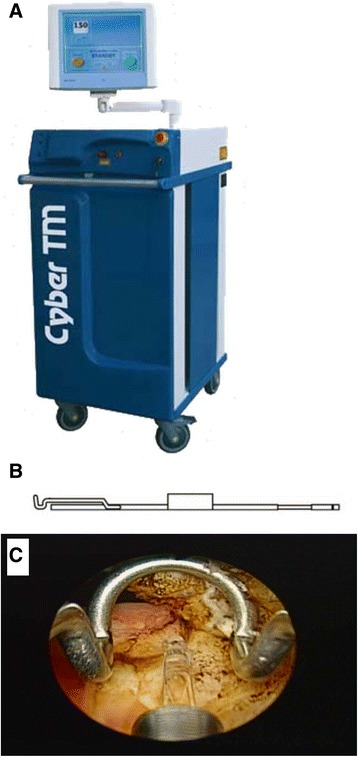
Background: Prostate vaporization and enucleation is a novel treatment option for bladder outlet obstruction caused by benign prostate enlargement. This surgical technique, however, has not yet been standardized. We present our findings of using a high-power thulium laser to accomplish vapoenucleation of the prostate (ThuVEP).
Methods: We prospectively collected and analyzed data from 29 patients who underwent ThuVEP between August 2010 and May 2012. The control group included 30 patients who underwent traditional transurethral resection of the prostate (TURP). Operative variables, patient profiles, preoperative and postoperative urine flow rates, prostate volume (measured using transrectal ultrasonography), and the international prostate symptom score (IPSS) were recorded and analyzed using a two-tailed Student's t-test and analysis of variance.
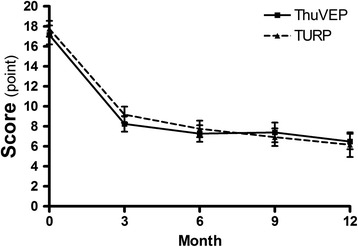
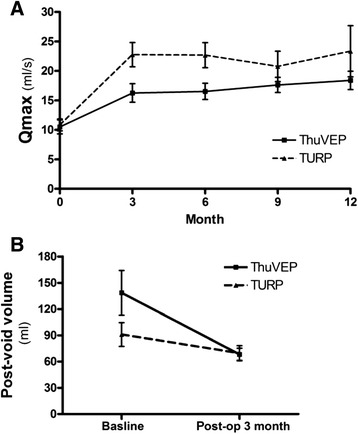
Results: The ages (mean ± SD) of the patients were 76.1 ± 9.4 and 72.6 ± 7.4 years (p = 0.28) in the ThuVEP and TURP groups, respectively. The average urinary flow rates before and 12 months after the operation (volume/maximum flow/average flow) were 243.3/10.5/5.0 and 302.8/17.6/9.4 (in mL, mL/s, mL/s, respectively) in the ThuVEP group and 247.2/10.8/4.6 and 369.9/20.8/12.0, respectively, in the TURP group. Preoperative and postoperative IPSSs were 17.1 ± 5.0 and 6.5 ± 3.8, respectively, in the ThuVEP group and 18.2 ± 4.5 and 6.2 ± 3.3, respectively, in the TURP group. The mean ratio of the estimated postoperative residual prostate volume to the preoperative total volume was 0.47 (p = 0.449) in both groups. The overall complication rate was 20.7% in the ThuVEP group and 30.0% in the TURP group.
Conclusions: One year of follow-up showed that ThuVEP and TURP effectively alleviated subjective and objective voiding symptoms with a low rate of complications. Thus, vapoenucleation using a high-power laser is feasible in elderly patients.
Trial registration: ISRCTN registry with study ID ISRCTN52339705 . Date assigned: 06/03/2015.
Figures
References
-
- Lo KL, Chan MC, Wong A, Hou SM, Ng CF. Long-term outcome of patients with a successful trial without catheter, after treatment with an alpha-adrenergic receptor blocker for acute urinary retention caused by benign prostatic hyperplasia. Int Urol Nephrol. 2010;42:7–12. doi: 10.1007/s11255-009-9572-7. - DOI - PubMed
-
- Flanigan RC, Reda DJ, Wasson JH, Anderson RJ, Abdellatif M, Bruskewitz RC. 5-year outcome of surgical resection and watchful waiting for men with moderately symptomatic benign prostatic hyperplasia: a department of veterans affairs cooperative study. J Urol. 1998;160:12–6. doi: 10.1016/S0022-5347(01)63011-8. - DOI - PubMed
-
- Hoekstra RJ, Van Melick HH, Kok ET, Ruud Bosch JL. A 10-year follow-up after transurethral resection of the prostate, contact laser prostatectomy and electrovaporization in men with benign prostatic hyperplasia; long-term results of a randomized controlled trial. BJU Int. 2010;106:822–6. doi: 10.1111/j.1464-410X.2010.09229.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
