

Utility of a novel inflammatory marker, GlycA, for assessment of rheumatoid arthritis disease activity and coronary atherosclerosis
- PMID: 25956924
- PMCID: PMC4445500
- DOI: 10.1186/s13075-015-0646-x
Utility of a novel inflammatory marker, GlycA, for assessment of rheumatoid arthritis disease activity and coronary atherosclerosis
Abstract
Introduction: GlycA is a novel inflammatory biomarker measured using nuclear magnetic resonance (NMR). Its NMR signal primarily represents glycosylated acute phase proteins. GlycA was associated with inflammation and development of cardiovascular disease in initially healthy women. We hypothesized that GlycA is a biomarker of disease activity and is associated with coronary artery atherosclerosis in patients with rheumatoid arthritis (RA).
Methods: We conducted a cross-sectional study of 166 patients with RA and 90 control subjects. GlycA was measured from an NMR signal originating from N-acetylglucosamine residues on circulating glycoproteins. The relationship between GlycA and RA disease activity (Disease Activity Score based on 28 joints (DAS28)) and coronary artery calcium score was determined.
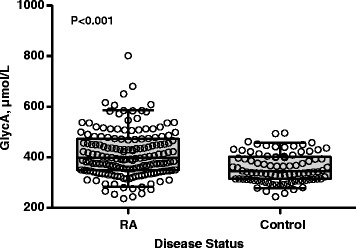
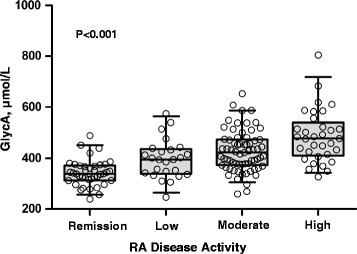
Results: GlycA concentrations were higher in patients with RA (median (interquartile range): 398 μmol/L (348 to 473 μmol/L)) than control subjects (344 μmol/L (314 to 403 μmol/L) (P < 0.001). In RA, GlycA was strongly correlated with DAS28 based on erythrocyte sedimentation rate (DAS28-ESR) and DAS28 based on C-reactive protein (DAS28-CRP) and their components, including tender and swollen joint counts, global health score, ESR and CRP (all P < 0.001). The area under the receiver operating characteristic curve for GlycA's ability to differentiate between patients with low versus moderate to high disease activity based on DAS28-CRP was 0.75 (95% confidence interval (CI): 0.68, 0.83). For each quartile increase in GlycA, the odds of having coronary artery calcium increased by 48% (95% CI: 4%, 111%), independent of age, race and sex (P = 0.03).
Conclusion: GlycA is a novel inflammatory marker that may be useful for assessment of disease activity and is associated with coronary artery atherosclerosis in patients with RA.
Figures
References
-
- van Leeuwen MA, van der Heijde DM, van Rijswijk MH, Houtman PM, van Riel PL, van de Putte LB, et al. Interrelationship of outcome measures and process variables in early rheumatoid arthritis: a comparison of radiologic damage, physical disability, joint counts, and acute phase reactants. J Rheumatol. 1994;21:425–9. - PubMed
-
- Smolen JS, Aletaha D, Bijlsma JW, Breedveld FC, Boumpas D, Burmester G, et al. Treating rheumatoid arthritis to target: recommendations of an international task force. Ann Rheum Dis. 2010;69:631–7. A published erratum appears in. Ann Rheum Dis. 2011;70:1519. doi: 10.1136/annrheumdis-2011-70-08. - DOI - PMC - PubMed
-
- Prevoo ML, van’t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts: development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38:44–8. doi: 10.1002/art.1780380107. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
