

Improved visualization of breast cancer features in multifocal carcinoma using phase-contrast and dark-field mammography: an ex vivo study
- PMID: 25956934
- PMCID: PMC4636518
- DOI: 10.1007/s00330-015-3773-5
Improved visualization of breast cancer features in multifocal carcinoma using phase-contrast and dark-field mammography: an ex vivo study
Abstract
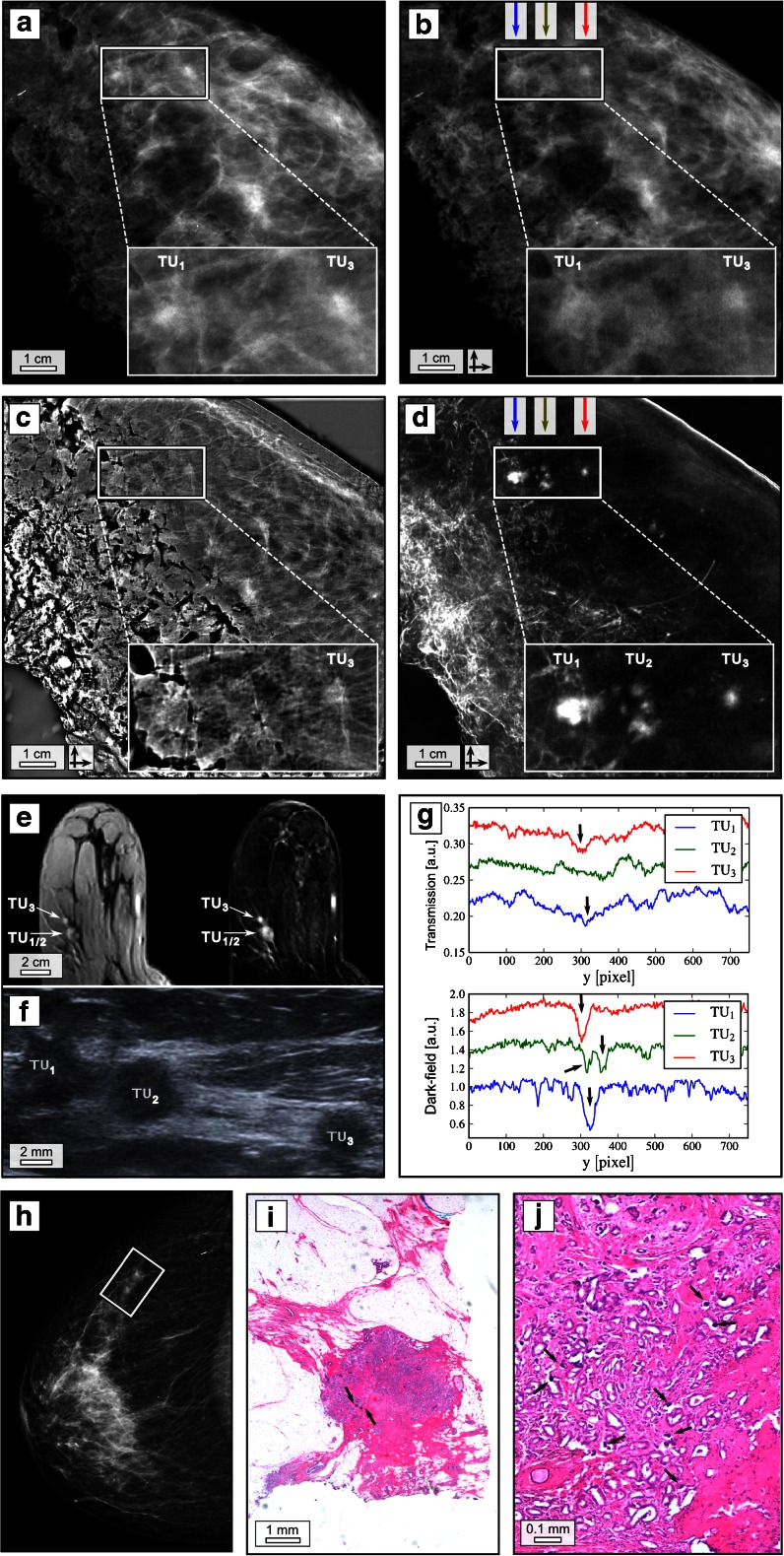
Objectives: Conventional X-ray attenuation-based contrast is inherently low for the soft-tissue components of the female breast. To overcome this limitation, we investigate the diagnostic merits arising from dark-field mammography by means of certain tumour structures enclosed within freshly dissected mastectomy samples.
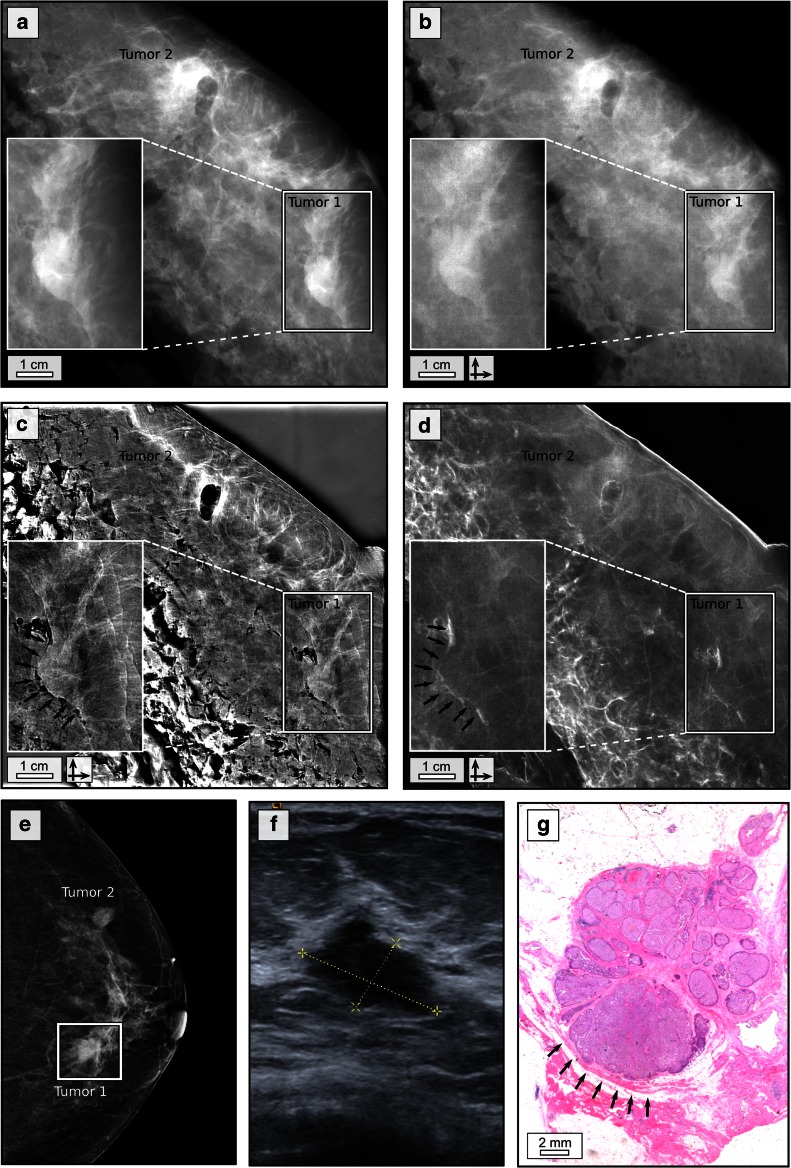
Methods: We performed grating-based absorption, absolute phase and dark-field mammography of three freshly dissected mastectomy samples containing bi- and multifocal carcinoma using a compact, laboratory Talbot-Lau interferometer. Preoperative in vivo imaging (digital mammography, ultrasound, MRI), postoperative histopathological analysis and ex vivo digital mammograms of all samples were acquired for the diagnostic verification of our results.
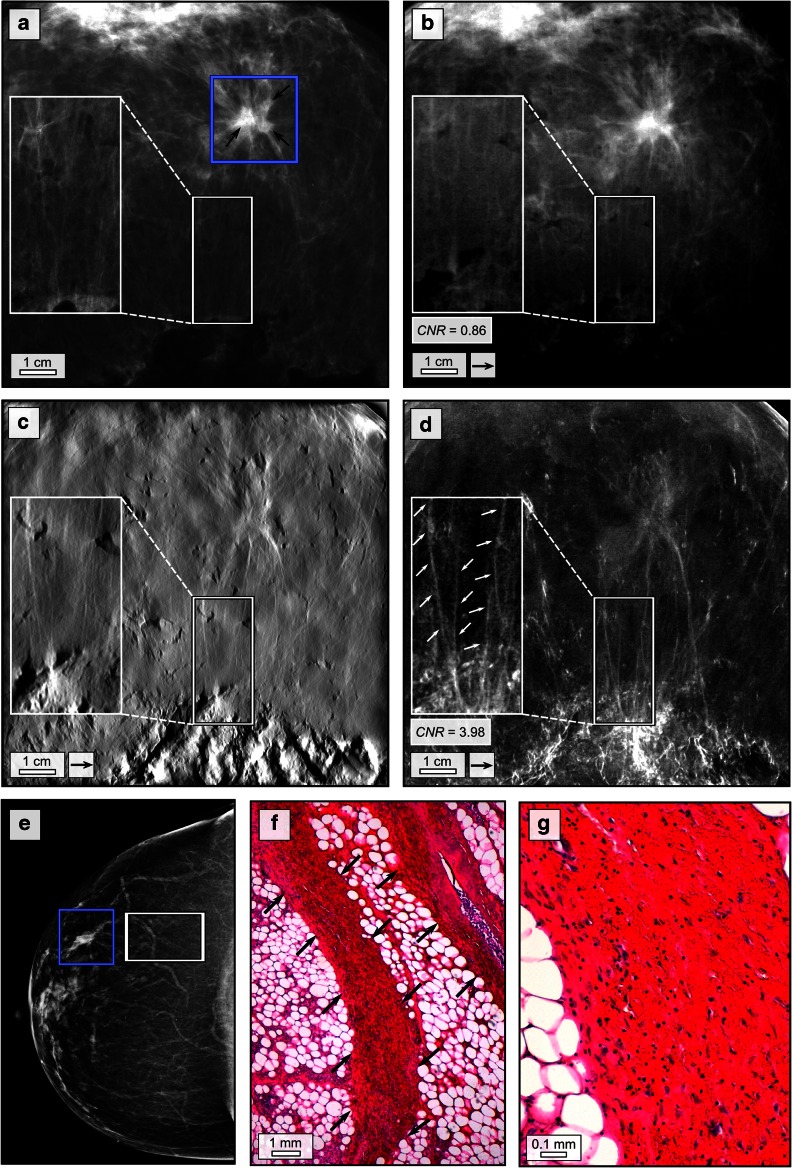
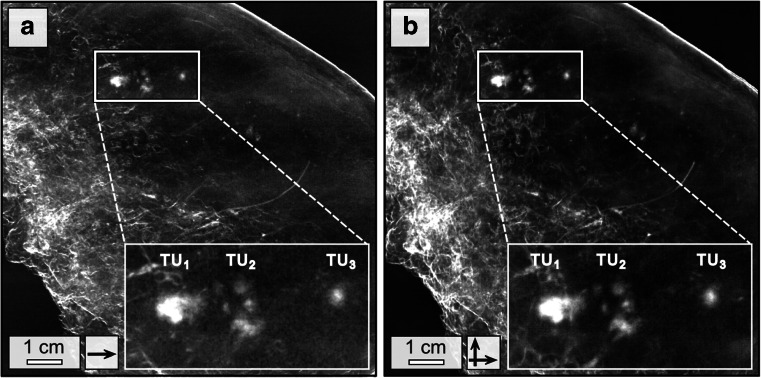
Results: In the diagnosis of multifocal tumour growth, dark-field mammography seems superior to standard breast imaging modalities, providing a better resolution of small, calcified tumour nodules, demarcation of tumour boundaries with desmoplastic stromal response and spiculated soft-tissue strands extending from an invasive ductal breast cancer.
Conclusions: On the basis of selected cases, we demonstrate that dark-field mammography is capable of outperforming conventional mammographic imaging of tumour features in both calcified and non-calcified tumours. Presuming dose optimization, our results encourage further studies on larger patient cohorts to identify those patients that will benefit the most from this promising additional imaging modality.
Key points: • X-ray dark-field mammography provides significantly improved visualization of tumour features • X-ray dark-field mammography is capable of outperforming conventional mammographic imaging • X-ray dark-field mammography provides imaging sensitivity towards highly dispersed calcium grains.
Keywords: Breast cancer; Grating interferometry; Mammography; X-ray dark-field imaging; X-ray phase-contrast imaging.
Figures
Similar articles
-
X-ray phase-contrast tomosynthesis for improved breast tissue discrimination.Eur J Radiol. 2014 Mar;83(3):531-6. doi: 10.1016/j.ejrad.2013.12.005. Epub 2013 Dec 12. Eur J Radiol. 2014. PMID: 24387825
-
On a dark-field signal generated by micrometer-sized calcifications in phase-contrast mammography.Phys Med Biol. 2013 Apr 21;58(8):2713-32. doi: 10.1088/0031-9155/58/8/2713. Epub 2013 Apr 3. Phys Med Biol. 2013. PMID: 23552903
-
Grating-based x-ray dark-field mammography: Assessing complementary imaging information in simple cystic lesions and typical fibroadenoma.Med Phys. 2025 Apr;52(4):2145-2154. doi: 10.1002/mp.17603. Epub 2025 Jan 3. Med Phys. 2025. PMID: 39752625 Free PMC article.
-
[Phase contrast imaging of the breast. Basic principles and steps towards clinical implementation].Radiologe. 2014 Mar;54(3):254-61. doi: 10.1007/s00117-013-2577-3. Radiologe. 2014. PMID: 24623010 Review. German.
-
Recent advances in X-ray imaging of breast tissue: From two- to three-dimensional imaging.Phys Med. 2020 Nov;79:69-79. doi: 10.1016/j.ejmp.2020.10.025. Epub 2020 Nov 7. Phys Med. 2020. PMID: 33171371 Review.
Cited by
-
Visualization of neonatal lung injury associated with mechanical ventilation using x-ray dark-field radiography.Sci Rep. 2016 Apr 13;6:24269. doi: 10.1038/srep24269. Sci Rep. 2016. PMID: 27072871 Free PMC article.
-
X-ray dark-field computed tomography for monitoring of tissue freezing.Sci Rep. 2024 Mar 7;14(1):5599. doi: 10.1038/s41598-024-56201-3. Sci Rep. 2024. PMID: 38454107 Free PMC article.
-
Dose-compatible grating-based phase-contrast mammography on mastectomy specimens using a compact synchrotron source.Sci Rep. 2018 Oct 24;8(1):15700. doi: 10.1038/s41598-018-33628-z. Sci Rep. 2018. PMID: 30356116 Free PMC article.
-
Hard X-ray omnidirectional differential phase and dark-field imaging.Proc Natl Acad Sci U S A. 2021 Mar 2;118(9):e2022319118. doi: 10.1073/pnas.2022319118. Proc Natl Acad Sci U S A. 2021. PMID: 33619105 Free PMC article.
-
[X‑ray Phase Contrast : Principles, potential and advances in clinical translation].Radiologe. 2018 Mar;58(3):218-225. doi: 10.1007/s00117-018-0357-9. Radiologe. 2018. PMID: 29374312 Review. German.
References
-
- Pinsky RW, Helvie MA. Mammographic breast density: effect on imaging and breast cancer risk. J Natl Compr Cancer. 2010;8:1157–1164. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
