

Epidemiology, Diagnosis, and Management of Esophageal Adenocarcinoma
- PMID: 25957861
- PMCID: PMC4516638
- DOI: 10.1053/j.gastro.2015.04.053
Epidemiology, Diagnosis, and Management of Esophageal Adenocarcinoma
Abstract
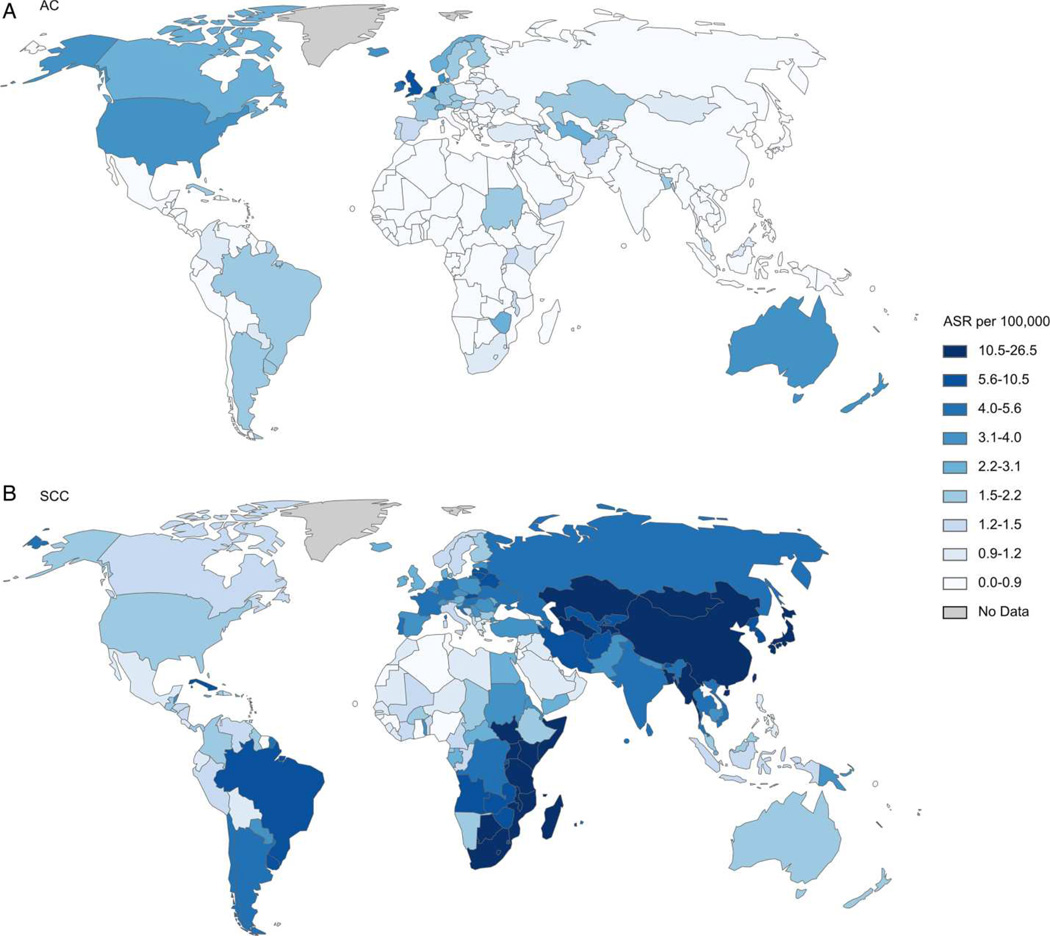
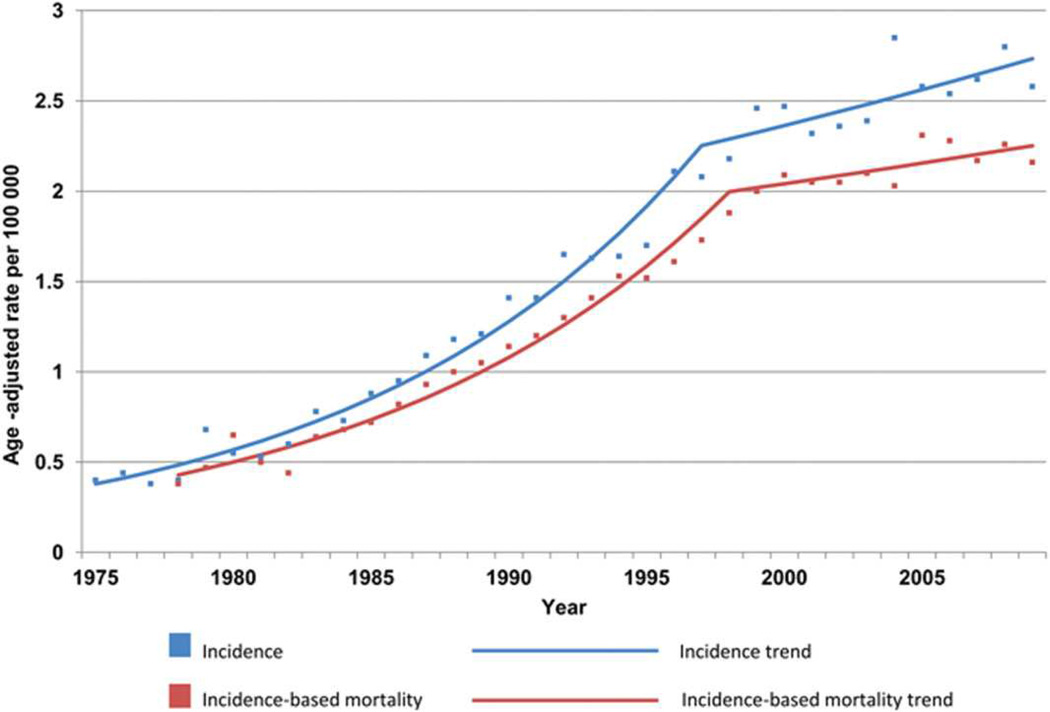
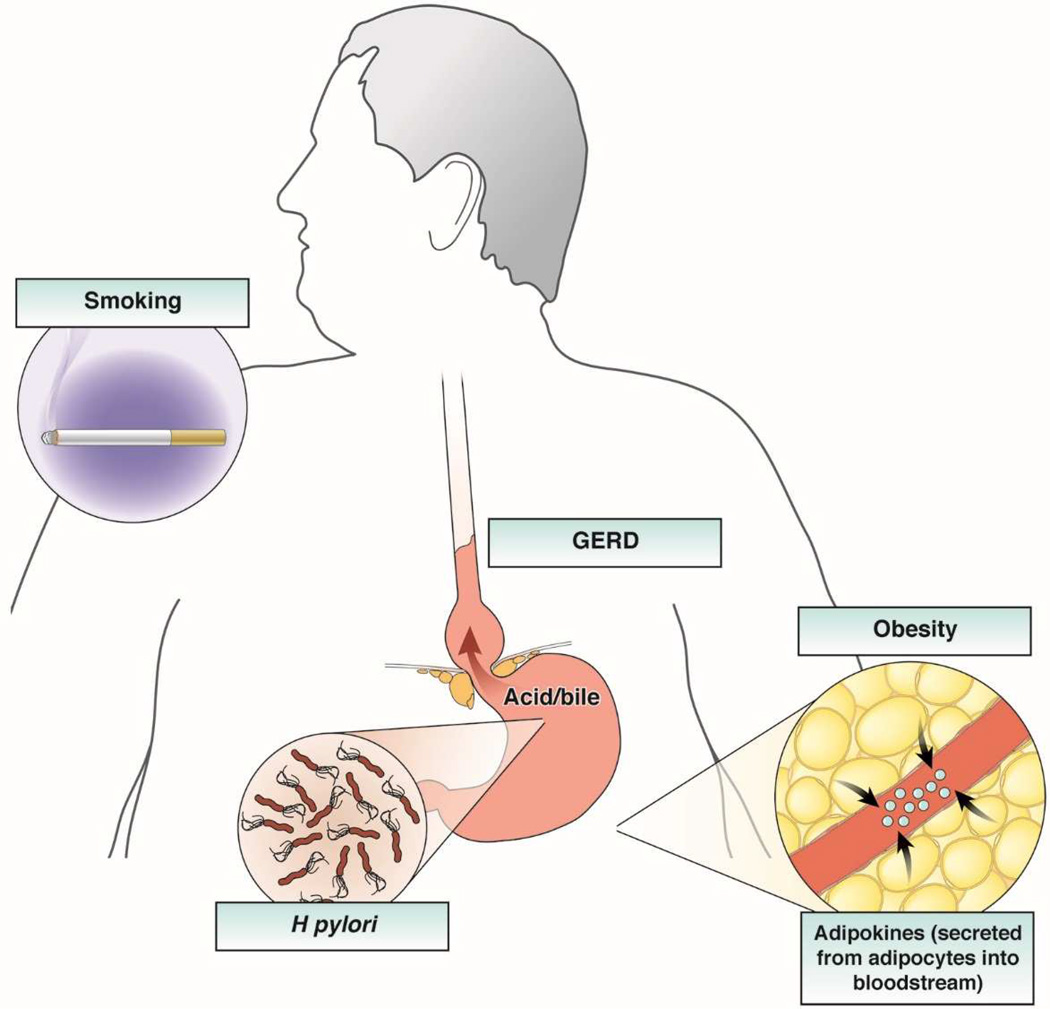
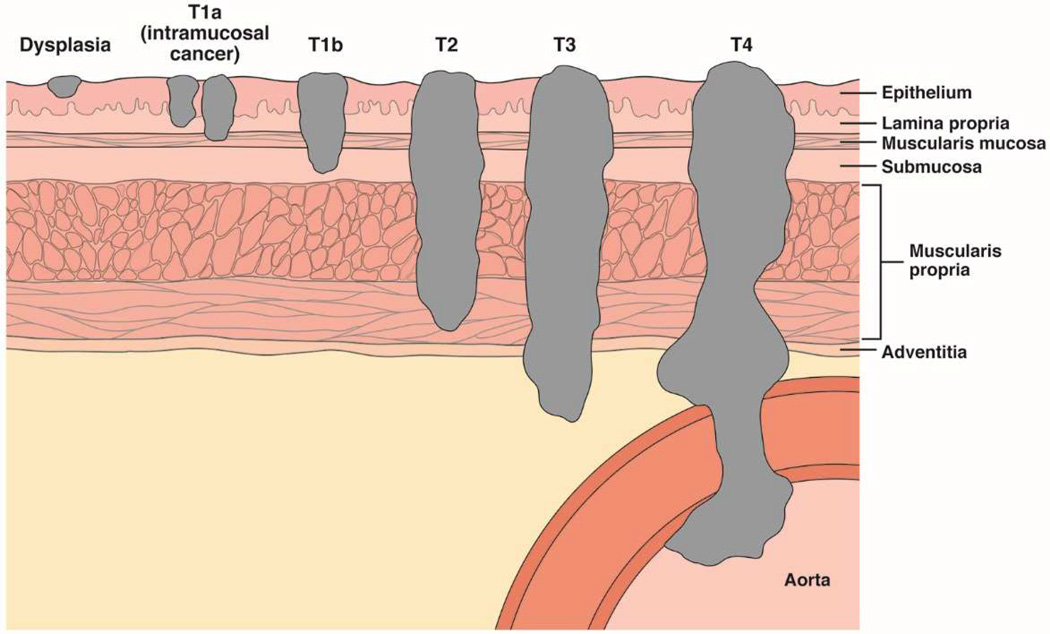
Esophageal adenocarcinoma (EAC) is rapidly increasing in incidence in Western cultures. Barrett's esophagus is the presumed precursor lesion for this cancer. Several other risk factors for this cancer have been described, including chronic heartburn, tobacco use, white race, and obesity. Despite these known associations, most patients with EAC present with symptoms of dysphagia from late-stage tumors; only a small number of patients are identified by screening and surveillance programs. Diagnostic analysis of EAC usually commences with upper endoscopy followed by cross-sectional imaging. Endoscopic ultrasonography is useful to assess the local extent of disease as well as the involvement of regional lymph nodes. T1a EAC may be treated endoscopically, and some patients with T1b disease may also benefit from endoscopic therapy. Locally advanced disease is generally managed with esophagectomy, often accompanied by neoadjuvant chemoradiotherapy or chemotherapy. The prognosis is based on tumor stage; patients with T1a tumors have an excellent prognosis, whereas few patients with advanced disease have long-term survival.
Keywords: Adenocarcinoma; Endoscopic Therapy; Esophageal Neoplasms; Risk Factors.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Surveillance, Epidemiology, and End Results (SEER) Program ( www.seer.cancer.gov) SEER*Stat Database: Incidence - SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov 2013 Sub (2000–2011) <Katrina/Rita Population Adjustment> - Linked To County Attributes - Total U.S., 1969–2012 Counties.: National Cancer Institute, DCCPS, Surveillance Research Program. Cancer Statistics Branch. Released April 2014 (updated 5/7/2014), based on the November 2013 submission.
-
- Trivers KF, Sabatino SA, Stewart SL, et al. Trends in esophageal cancer incidence by histology, United States, 1998–2003. International Journal of Cancer. 2008;123:1422–1428. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF., Jr Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83:2049–2053. - PubMed
-
- National Cancer Institute. Surveillance, Epidemiology and End Results (SEER) Program. [accessed January 9, 2015];Esophagus Table 8.22. www.seer.cancer.gov/csr/1975_2010/browse_csr.php.
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
