

Knowledge-based radiation therapy (KBRT) treatment planning versus planning by experts: validation of a KBRT algorithm for prostate cancer treatment planning
- PMID: 25957871
- PMCID: PMC4433067
- DOI: 10.1186/s13014-015-0416-6
Knowledge-based radiation therapy (KBRT) treatment planning versus planning by experts: validation of a KBRT algorithm for prostate cancer treatment planning
Abstract
Background: A knowledge-based radiation therapy (KBRT) treatment planning algorithm was recently developed. The purpose of this work is to investigate how plans that are generated with the objective KBRT approach compare to those that rely on the judgment of the experienced planner.
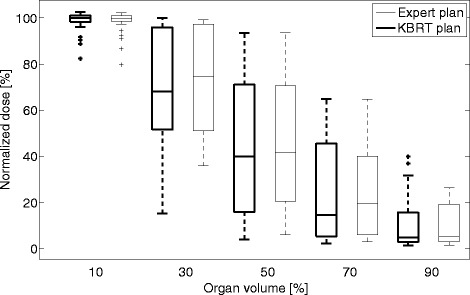
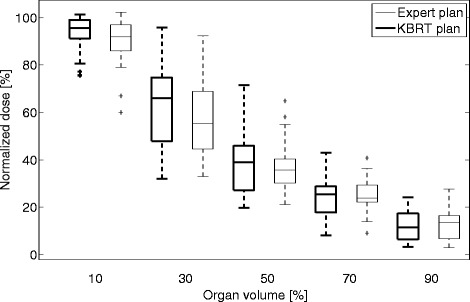
Methods: Thirty volumetric modulated arc therapy plans were randomly selected from a database of prostate plans that were generated by experienced planners (expert plans). The anatomical data (CT scan and delineation of organs) of these patients and the KBRT algorithm were given to a novice with no prior treatment planning experience. The inexperienced planner used the knowledge-based algorithm to predict the dose that the OARs receive based on their proximity to the treated volume. The population-based OAR constraints were changed to the predicted doses. A KBRT plan was subsequently generated. The KBRT and expert plans were compared for the achieved target coverage and OAR sparing. The target coverages were compared using the Uniformity Index (UI), while 5 dose-volume points (D10, D30, D50, D70 and D90) were used to compare the OARs (bladder and rectum) doses. Wilcoxon matched-pairs signed rank test was used to check for significant differences (p<0.05) between both datasets.
Results: The KBRT and expert plans achieved mean UI values of 1.10 ± 0.03 and 1.10 ± 0.04, respectively. The Wilcoxon test showed no statistically significant difference between both results. The D90, D70, D50, D30 and D10 values of the two planning strategies, and the Wilcoxon test results suggests that the KBRT plans achieved a statistically significant lower bladder dose (at D30), while the expert plans achieved a statistically significant lower rectal dose (at D10 and D30).
Conclusions: The results of this study show that the KBRT treatment planning approach is a promising method to objectively incorporate patient anatomical variations in radiotherapy treatment planning.
Figures
References
-
- Good D, Lo J, Lee WR, Wu QJ, Yin F-F, Das SK. A knowledge-based approach to improving and homogenizing intensity modulated radiation therapy planning quality among treatment centers: an example application to prostate cancer planning. Int J Radiat Oncol, Biol, Phys. 2013;87(1):176–181. doi: 10.1016/j.ijrobp.2013.03.015. - DOI - PubMed
-
- Wang Y, Zolnay A, Incrocci L, Joosten H, McNutt T, Heijmen B, et al. A quality control model that uses PTV-rectal distances to predict the lowest achievable rectum dose, improves IMRT planning for patients with prostate cancer. Radiother Oncol. 2013;107(3):352–357. doi: 10.1016/j.radonc.2013.05.032. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
