

50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study
- PMID: 25960110
- PMCID: PMC4553037
- DOI: 10.1016/S0140-6736(14)61774-8
50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study
Abstract
Background: Comprehensive long-term data on atrial fibrillation trends in men and women are scant. We aimed to provide such data through analysis of the Framingham cohort over 50 years.
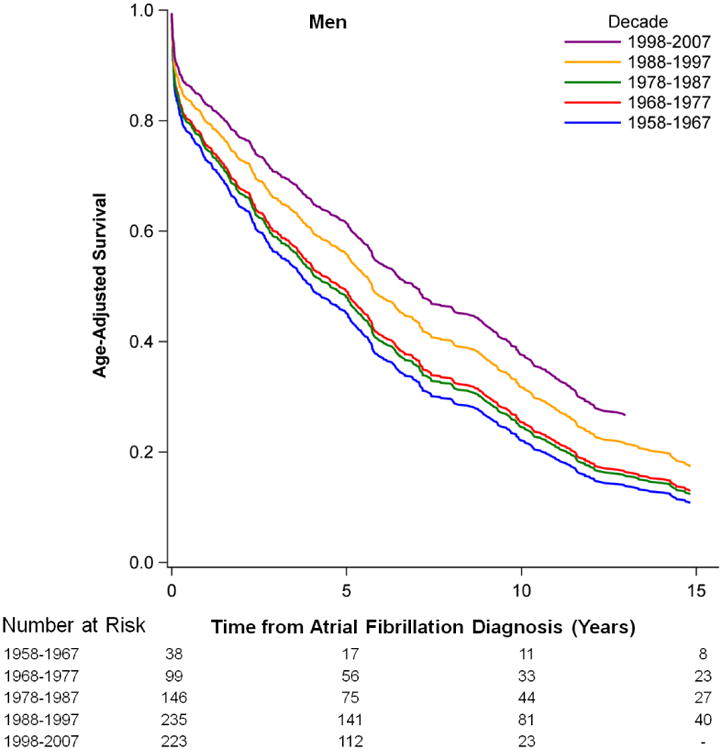
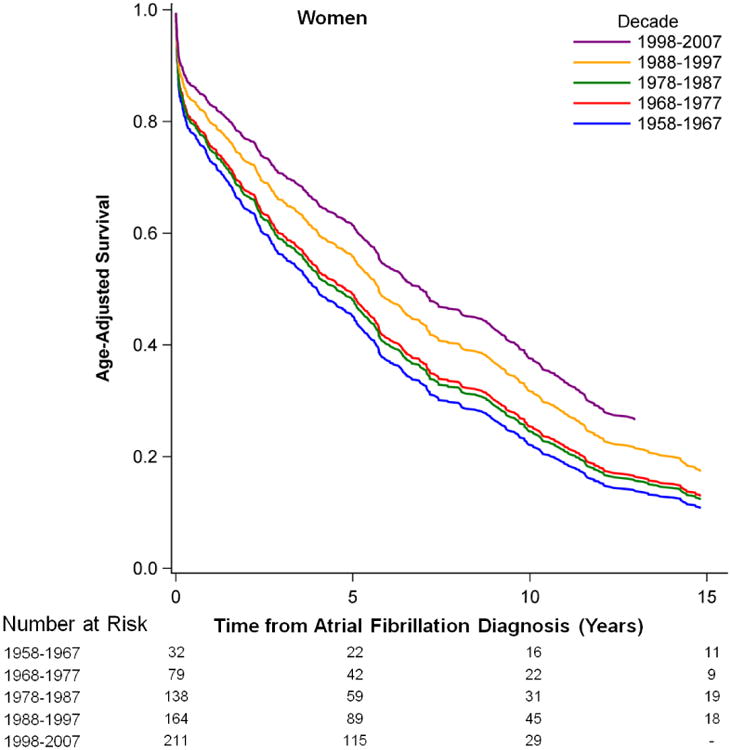
Methods: We investigated trends in incidence, prevalence, and risk factors for atrial fibrillation and its association with stroke and mortality after onset in 9511 participants enrolled in the Framingham Heart Study between 1958 and 2007. We analysed trends within 10 year groups (1958-67, 1968-77, 1978-87, 1988-97, and 1998-2007), stratified by sex.
Findings: During 50 years of observation (202,417 person-years), 1544 cases of new-onset atrial fibrillation occurred (of whom 723 [47%] were women). Between 1958-67 and 1998-2007, age-adjusted prevalence of atrial fibrillation quadrupled from 20·4 to 96·2 cases per 1000 person-years in men and from 13·7 to 49·4 cases per 1000 person-years in women; age-adjusted incidence increased from 3·7 to 13·4 new cases per 1000 person-years in men and from 2·5 to 8·6 new cases per 1000 person-years in women (ptrend<0·0001 for all comparisons). For atrial fibrillation diagnosed by electrocardiograph (ECG) during routine Framingham examinations, age-adjusted prevalence per 1000 person-years increased (12·6 in 1958-67 to 25·7 in 1998-2007 in men, ptrend=0·0007; 8·1 to 11·8 in women, ptrend=0·009). However, age-adjusted incidence of atrial fibrillation by Framingham Heart Study ECGs did not change significantly with time. Although the prevalence of most risk factors changed over time, their associated hazards for atrial fibrillation changed little. Multivariable-adjusted proportional hazards models revealed a 74% (95% CI 50-86%) decrease in stroke (hazards ratio [HR] 3·77, 95% CI 1·98-7·20 in 1958-1967 compared with 1998-2007; ptrend=0·0001) and a 25% (95% CI -3-46%) decrease in mortality (HR 1·34, 95% CI 0·97-1·86 in 1958-1967 compared with 1998-2007; ptrend=0·003) in 20 years following atrial fibrillation onset.
Interpretation: Trends of increased incidence and prevalence of atrial fibrillation in the community were probably partly due to enhanced surveillance. Measures are needed to enhance early detection of atrial fibrillation, through increased awareness coupled with targeted screening programmes and risk factor-specific prevention.
Funding: NIH, NHLBI, NINDS, Deutsche Forschungsgemeinschaft.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Taking the pulse of atrial fibrillation.Lancet. 2015 Jul 11;386(9989):113-5. doi: 10.1016/S0140-6736(14)61991-7. Epub 2015 May 7. Lancet. 2015. PMID: 25960109 No abstract available.
References
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–25. - PubMed
-
- Wattigney WA, Mensah GA, Croft JB. Increased atrial fibrillation mortality: United States, 1980-1998. Am J Epidemiol. 2002;155:819–26. - PubMed
Publication types
MeSH terms
Grants and funding
- N01-HC-25195/HC/NHLBI NIH HHS/United States
- 1RC1HL101056/HL/NHLBI NIH HHS/United States
- K24 HL105780/HL/NHLBI NIH HHS/United States
- 1K23HL114724/HL/NHLBI NIH HHS/United States
- R01 HL104156/HL/NHLBI NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- R01 HL077477/HL/NHLBI NIH HHS/United States
- RC1 HL099452/HL/NHLBI NIH HHS/United States
- RC1 HL101056/HL/NHLBI NIH HHS/United States
- HL080124/HL/NHLBI NIH HHS/United States
- AG028321/AG/NIA NIH HHS/United States
- U01 HL105268/HL/NHLBI NIH HHS/United States
- R01 HL102214/HL/NHLBI NIH HHS/United States
- 1K24HL105780/HL/NHLBI NIH HHS/United States
- HL102214/HL/NHLBI NIH HHS/United States
- R01 HL093328/HL/NHLBI NIH HHS/United States
- P30 AG010129/AG/NIA NIH HHS/United States
- K23 HL114724/HL/NHLBI NIH HHS/United States
- R01 HL071039/HL/NHLBI NIH HHS/United States
- R01HL104156/HL/NHLBI NIH HHS/United States
- R01 NS017950/NS/NINDS NIH HHS/United States
- 2R01HL092577/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- KL2RR031981/RR/NCRR NIH HHS/United States
- 1U01HL105268-01/HL/NHLBI NIH HHS/United States
- R01 AG008122/AG/NIA NIH HHS/United States
- HL093328/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- 6R01-NS-17950/NS/NINDS NIH HHS/United States
- 1R01HL102214/HL/NHLBI NIH HHS/United States
- R01 HL080124/HL/NHLBI NIH HHS/United States
- 1R01AG028321/AG/NIA NIH HHS/United States
- R01 AG028321/AG/NIA NIH HHS/United States
- 1R01HL092577/HL/NHLBI NIH HHS/United States
- HL71039/HL/NHLBI NIH HHS/United States
- 2014105/DDCF/Doris Duke Charitable Foundation/United States
- KL2 RR031981/RR/NCRR NIH HHS/United States
- K23 HL080025/HL/NHLBI NIH HHS/United States
- HL080025/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
