

Management of Coronary Artery Calcium and Coronary CTA Findings
- PMID: 25960825
- PMCID: PMC4412516
- DOI: 10.1007/s12410-015-9334-0
Management of Coronary Artery Calcium and Coronary CTA Findings
Abstract
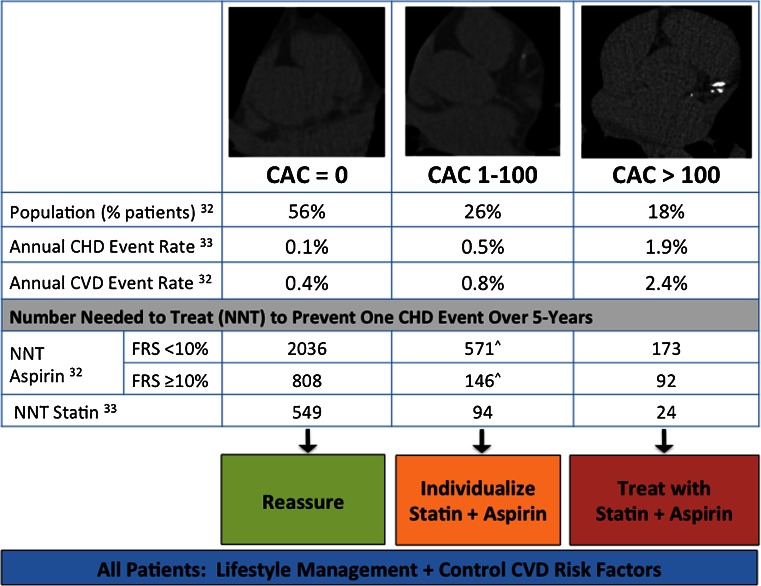
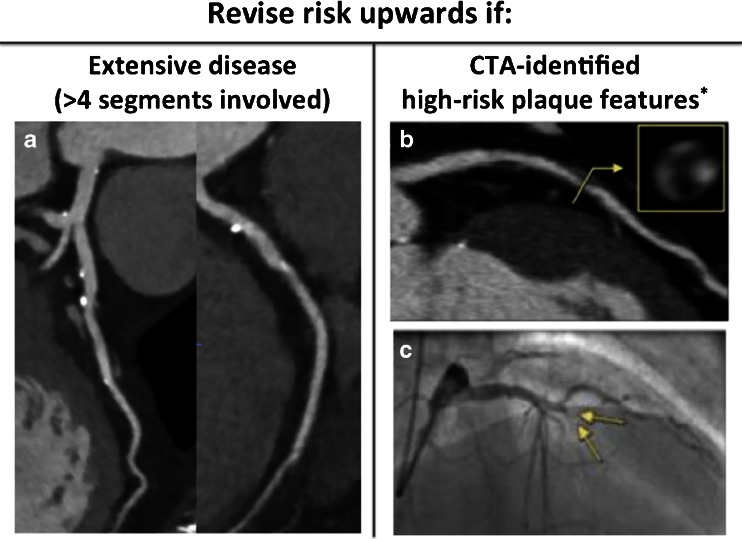
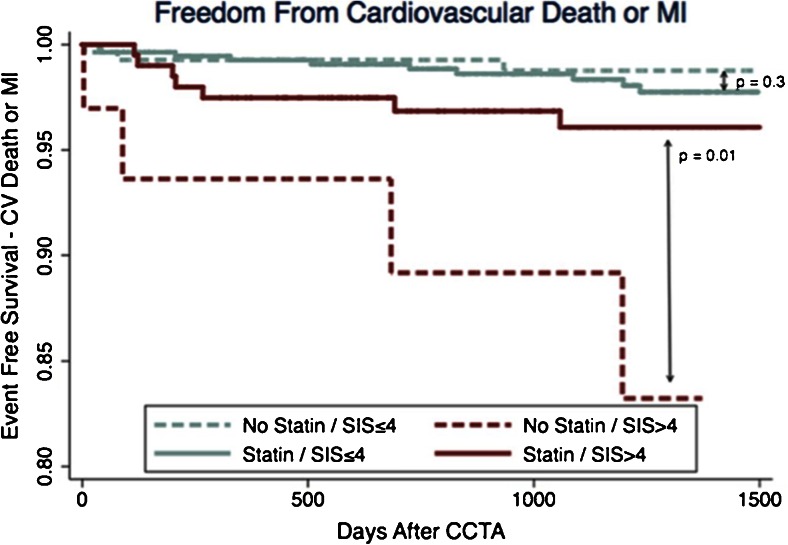
Coronary artery calcium (CAC) testing and coronary computed tomography angiography (CTA) have significant data supporting their ability to identify coronary artery disease (CAD) and classify patient risk for atherosclerotic cardiovascular disease (ASCVD). Evidence regarding CAC use for screening has established an excellent prognosis in patients with no detectable CAC, and the ability to risk re-classify the majority of asymptomatic patients considered intermediate risk by traditional risk scores. While data regarding the ideal management of CAC findings are limited, evidence supports statin consideration in patients with CAC > 0 and individualized aspirin therapy accounting for CAD risk factors, CAC severity, and factors which increase a patient's risk of bleeding. In patients with stable or acute symptoms undergoing coronary CTA, a normal CTA predicts excellent prognosis, allowing reassurance and disposition without further testing. When CTA identifies nonobstructive CAD (<50 % stenosis), observational data support consideration of statin use/intensification in patients with extensive plaque (at least four coronary segments involved) and patients with high-risk plaque features. In patients with both nonobstructive and obstructive CAD, multiple studies have now demonstrated an ability of CTA to guide management and improve CAD risk factor control. Still, significant under-treatment of cardiovascular risk factors and high-risk image findings remain, among concerns that CTA may increase invasive angiography and revascularization. To fully realize the impact of atherosclerosis imaging for ASCVD prevention, patient engagement in lifestyle changes and the modification of ASCVD risk factors remain the foundation of care. This review provides an overview of available data and recommendations in the management of CAC and CTA findings.
Keywords: Acute coronary syndrome; Cardiovascular disease; Chest pain; Coronary CTA; Coronary artery calcium; High risk plaque; Ischemic heart disease; Major adverse cardiac events; Management; Prognosis; atherosclerosis.
Figures



References
-
- Xu J, Kochanek KD, Murphy SL, Arias E. Mortality in the United States, 2012. NCHS Data Brief. 2014;(168):1–8. - PubMed
-
- Crescioni M, Gorina Y, Bilheimer L, Gillum RF. Trends in health status and health care use among older men. Natl Health Stat Report. 2010;(24):1–18. - PubMed
-
- Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670–81. doi: 10.1016/S0140-6736(10)61350-5. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous