

Regional versus General Anesthesia for Percutaneous Nephrolithotomy: A Meta-Analysis
- PMID: 25961831
- PMCID: PMC4427359
- DOI: 10.1371/journal.pone.0126587
Regional versus General Anesthesia for Percutaneous Nephrolithotomy: A Meta-Analysis
Abstract
Objective: To compare the effectiveness and safety of regional anesthesia (RA) and general anesthesia (GA) for percutaneous nephrolithotomy (PNL).
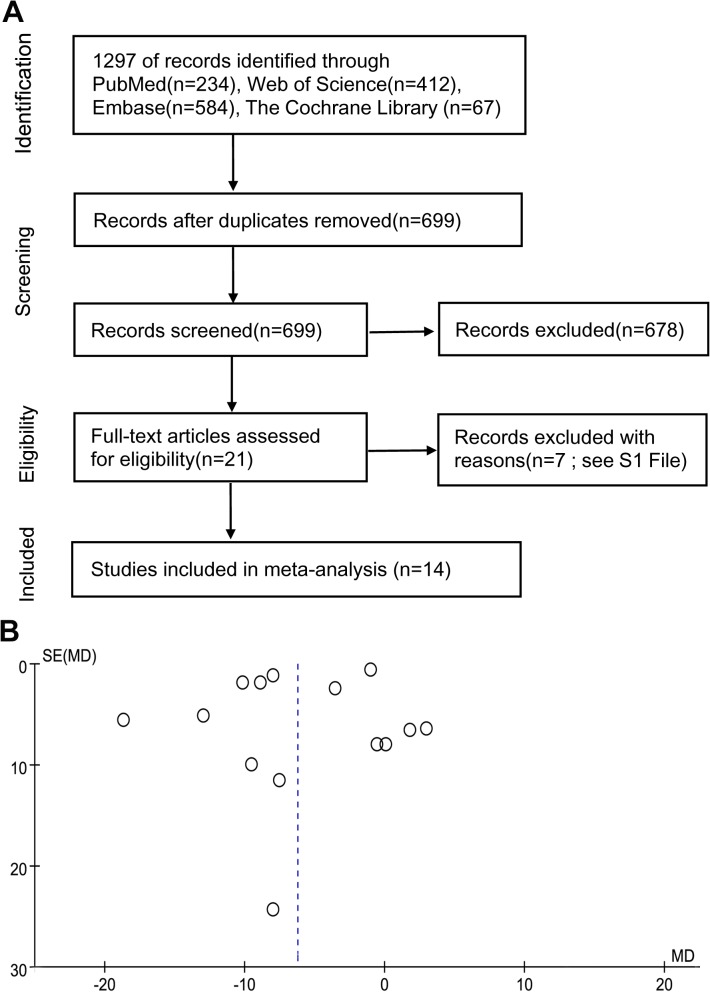
Patients and methods: PubMed, EMBASE, The Cochrane Library, and the Web of Knowledge databases were systematically searched to identify relevant studies. After literature screening and data extraction, a meta-analysis was performed using the RevMan 5.3 software.
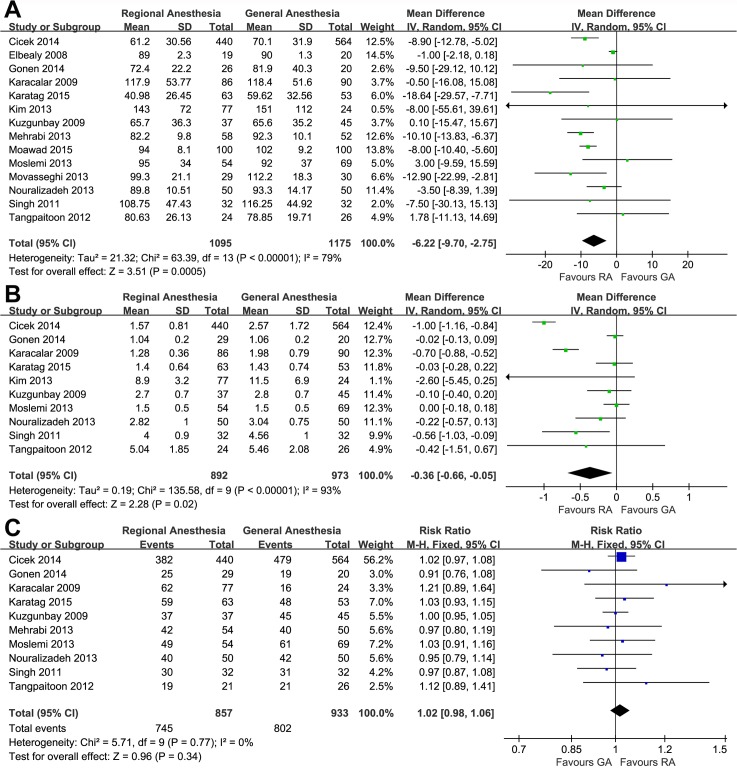
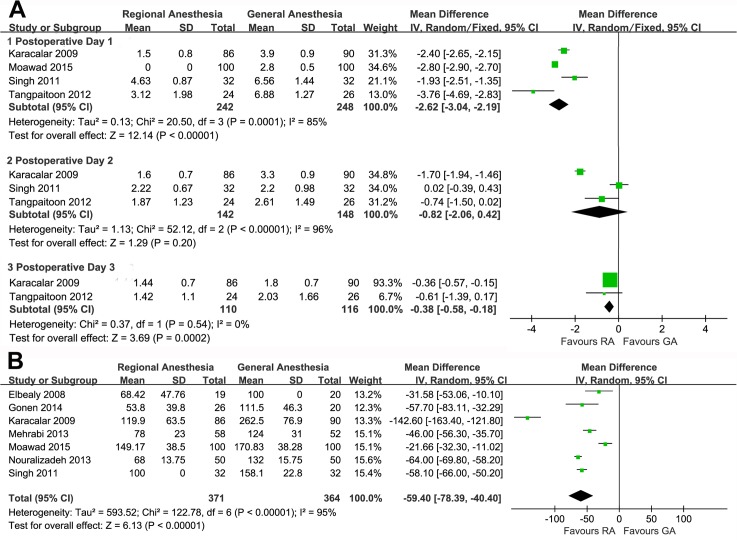
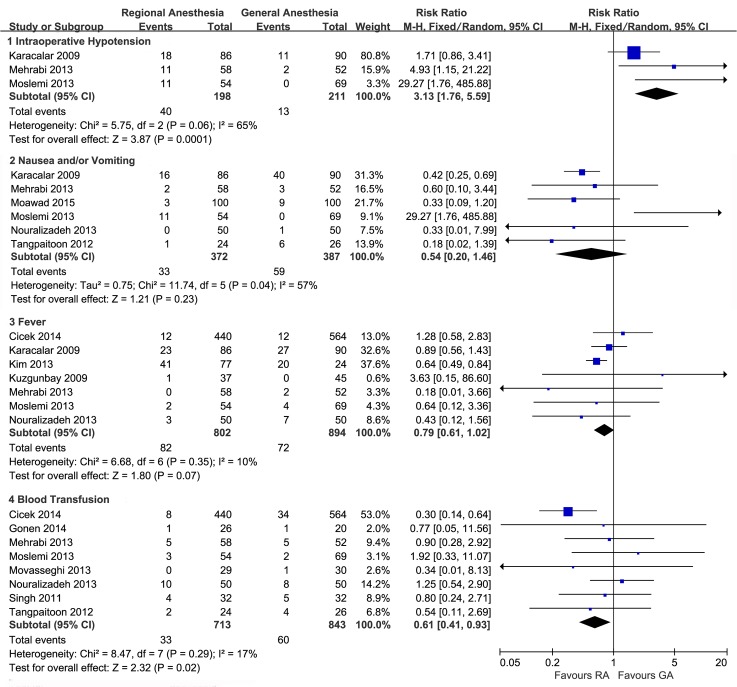
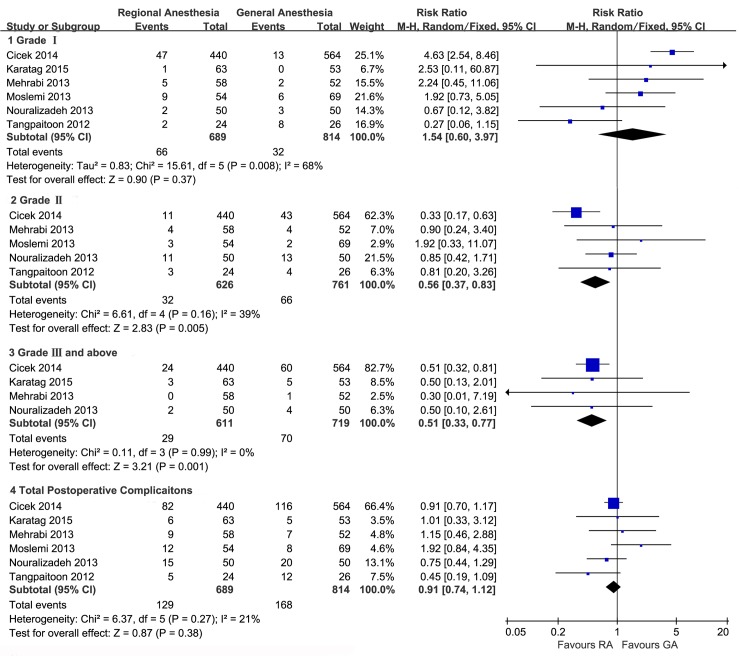
Results: Eight randomized controlled trials (RCTs) and six non-randomized controlled trials (nRCTs) involving 2270 patients were included. Patients receiving RA were associated with shorter operative time (-6.22 min; 95%CI, -9.70 to -2.75; p = 0.0005), lower visual analgesic score on the first and third postoperative day (WMD, -2.62; 95%CI, -3.04 to -2.19; p < 0.00001 WMD, -0.38; 95%CI, -0.58 to -0.18; p = 0.0002), less analgesic requirements (WMD, -59.40 mg; 95%CI, -78.39 to -40.40; p<0.00001), shorter hospitalization (WMD, -0.36d; 95%CI, -0.66 to -0.05; p = 0.02), less blood transfusion (RR, 0.61; 95%CI, 0.41 to 0.93; p = 0.02), fewer modified Clavion-Dindo Grade II (RR, 0.56; 95%CI, 0.37 to 0.83; p = 0.005), Grade III or above postoperative complications (RR, 0.51; 95%CI, 0.33 to 0.77; p = 0.001), and potential benefits of less fever (RR, 0.79; 95%CI, 0.61 to 1.02; p = 0.07), nausea or vomiting (RR, 0.54; 95%CI, 0.20 to 1.46; p = 0.23), whereas more intraoperative hypotension (RR, 3.13; 95%CI, 1.76 to 5.59; p = 0.0001) when compared with patients receiving GA. When nRCTs were excluded, most of the results were stable but the significant differences were no longer detectable in blood transfusion, Grade II and more severe complications. No significant difference in the total postoperative complications and stone-free rate were found.
Conclusions: Current evidence suggests that both RA and GA can provide safe and effective anesthesia for PNL in carefully evaluated and selected patients. Each anesthesia technique has its own advantages but some aspects still remain unclear and need to be explored in future studies.
Conflict of interest statement
Figures
References
-
- Türk C, Knoll T, Petrik A, Sarica K, Skolarikos A, Straub M, et al. Guidelines on urolithiasis. Uroweb 2014 Available: http://www.uroweb.org/gls/pdf/22%20Urolithiasis_LRpdf. Accessed August 15, 2014.
-
- Preminger GM, Assimos DG, Lingeman JE, Nakada SY, Pearle MS, Wolf JS Jr, et al. AUA guideline on management of staghorn calculi: diagnosis and treatment recommendations. J Urol. 2005;173:1991–2000. - PubMed
-
- Singh I, Kumar A, Kumar P. "Ambulatory PCNL" (tubeless PCNL under regional anesthesia)—a preliminary report of 10 cases. Int Urol Nephrol. 2005;37:35–37. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
