

Cross-reactive and pre-existing antibodies to therapeutic antibodies--Effects on treatment and immunogenicity
- PMID: 25962087
- PMCID: PMC4623040
- DOI: 10.1080/19420862.2015.1048411
Cross-reactive and pre-existing antibodies to therapeutic antibodies--Effects on treatment and immunogenicity
Abstract
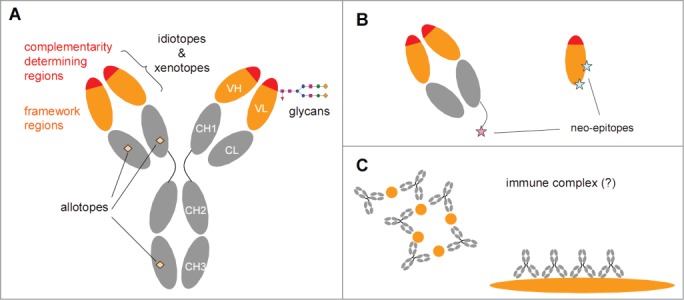
The potential for immunogenicity is an ever-present concern during the development of biopharmaceuticals. Therapeutic antibodies occasionally elicit an antibody response in patients, which can result in loss of response or adverse effects. However, antibodies that bind a drug are sometimes found in pre-treatment serum samples, with the amount depending on drug, assay, and patient population. This review summarizes published data on pre-existing antibodies to therapeutic antibodies, including rheumatoid factors, anti-allotype antibodies, anti-hinge antibodies, and anti-glycan antibodies. Unlike anti-idiotype antibodies elicited by the drug, pre-formed antibodies in general appear to have little consequences during treatment. In the few cases where (potential) clinical consequences were encountered, antibodies were characterized and found to bind a distinct, unusual epitope of the therapeutic. Immunogenicity testing strategies should therefore always include a proper level of antibody characterization, especially when pre-formed antibodies are present. This minimizes false-positives, particularly due to rheumatoid factors, and helps to judge the potential threat in case a genuine pre-dose antibody reactivity is identified.
Keywords: ADA, anti-drug antibody; CDR, complementarity-determining region; RA, rheumatoid arthritis; RF, rheumatoid factor; TNF, tumor necrosis factor; VH, variable heavy; VL, variable light; allotype; anti-drug antibodies (ADA); glycan; idiotype; immunogenicity; pre-existing antibodies; rheumatoid factor.
Figures
References
-
- Chatenoud L, Jonker M, Villemain F, Goldstein G, Bach JF. The human immune response to the OKT3 monoclonal antibody is oligoclonal. Science 1986; 232: 1406-1408; PMID:3086976; http://dx.doi.org/ 10.1126/science.3086976. - DOI - PubMed
-
- Knight DM, Wagner C, Jordan R, McAleer MF, DeRita R, Fass DN, Coller BS, Weisman HF, Ghrayeb J. The immunogenicity of the 7E3 murine monoclonal Fab antibody fragment variable region is dramatically reduced in humans by substitution of human for murine constant regions. Mol Immunol 1995; 32: 1271-1281; PMID:8559151; http://dx.doi.org/ 10.1016/0161-5890(95)00085-2. - DOI - PubMed
-
- Harding FA, Stickler MM, Razo J, DuBridge RB. The immunogenicity of humanized and fully human antibodies: residual immunogenicity resides in the CDR regions. MAbs 2010; 2: 256-265; PMID:20400861; http://dx.doi.org/ 10.4161/mabs.2.3.11641. - DOI - PMC - PubMed
-
- van Schouwenburg PA, Rispens T, Wolbink GJ. Immunogenicity of anti-TNF biologic therapies for rheumatoid arthritis. Nat Rev Rheumatol 2013; 9: 164-172; PMID:23399692; http://dx.doi.org/ 10.1038/nrrheum.2013.4. - DOI - PubMed
-
- Vincent FB, Morand EF, Murphy K, Mackay F, Mariette X, Marcelli C. Antidrug antibodies (ADAb) to tumour necrosis factor (TNF)-specific neutralising agents in chronic inflammatory diseases: a real issue, a clinical perspective. Ann Rheum Dis 2013; 72: 165-178; http://dx.doi.org/ 10.1136/annrheumdis-2012-202545. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials