

Body mass index and outcome in renal transplant recipients: a systematic review and meta-analysis
- PMID: 25963131
- PMCID: PMC4427990
- DOI: 10.1186/s12916-015-0340-5
Body mass index and outcome in renal transplant recipients: a systematic review and meta-analysis
Erratum in
-
Erratum: Body mass index and outcome in renal transplant recipients: a systematic review and meta-analysis.BMC Med. 2015 Jun 15;13:141. doi: 10.1186/s12916-015-0387-3. BMC Med. 2015. PMID: 26076728 Free PMC article.
Abstract
Background: Whether overweight or obese end stage renal disease (ESRD) patients are suitable for renal transplantation (RT) is often debated. The objective of this review and meta-analysis was to systematically investigate the outcome of low versus high BMI recipients after RT.
Methods: Comprehensive searches were conducted in MEDLINE OvidSP, Web of Science, Google Scholar, Embase, and CENTRAL (the Cochrane Library 2014, issue 8). We reviewed four major guidelines that are available regarding (potential) RT recipients. The methodology was in accordance with the Cochrane Handbook for Systematic Reviews of Interventions and written based on the PRISMA statement. The quality assessment of studies was performed by using the GRADE tool. A meta-analysis was performed using Review Manager 5.3. Random-effects models were used.
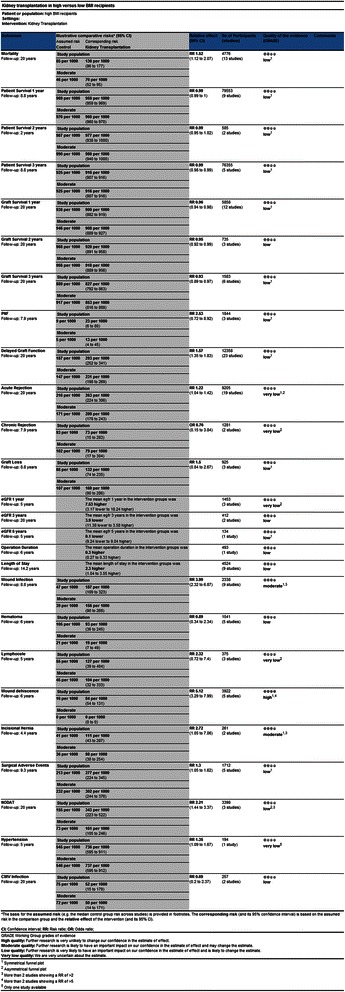
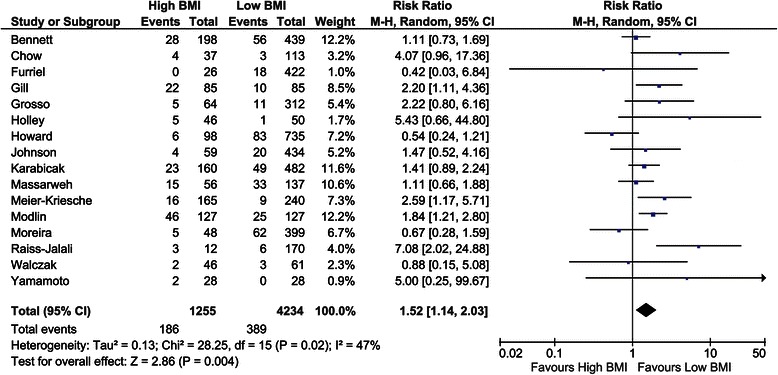
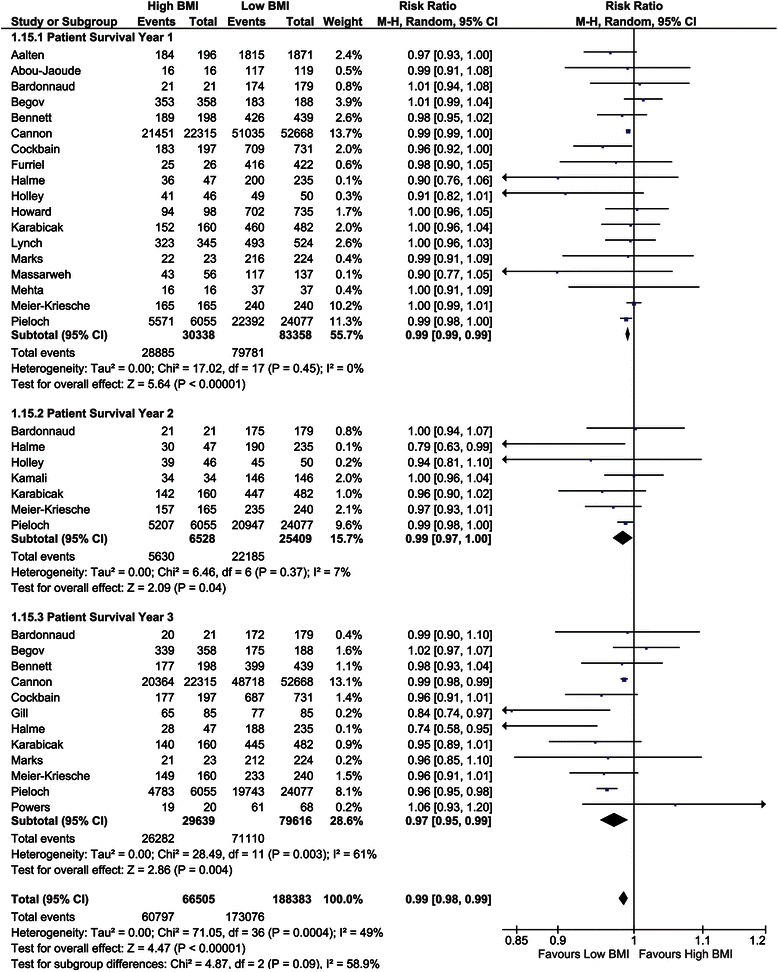
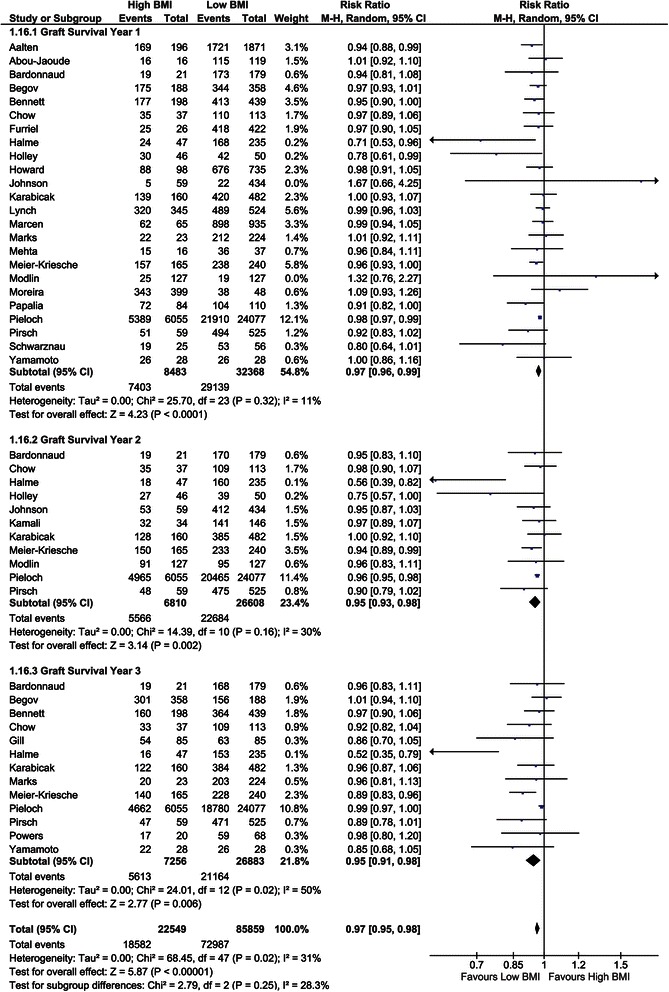
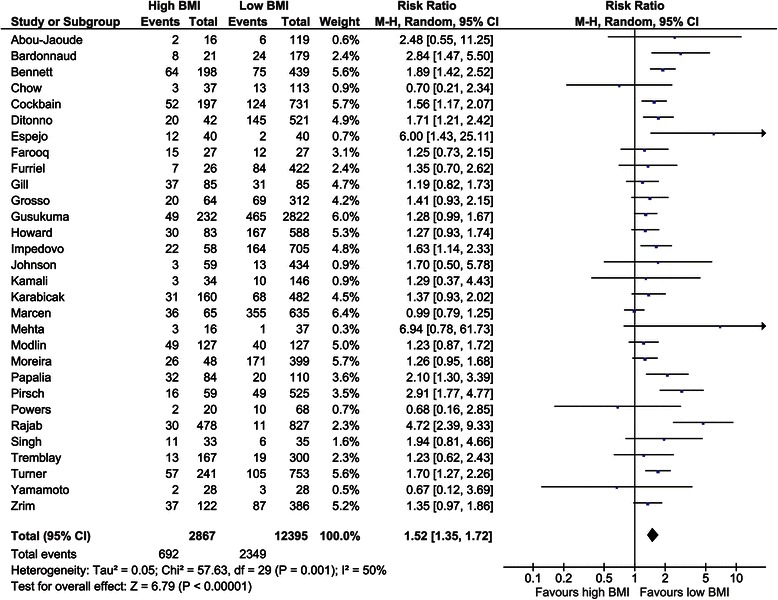
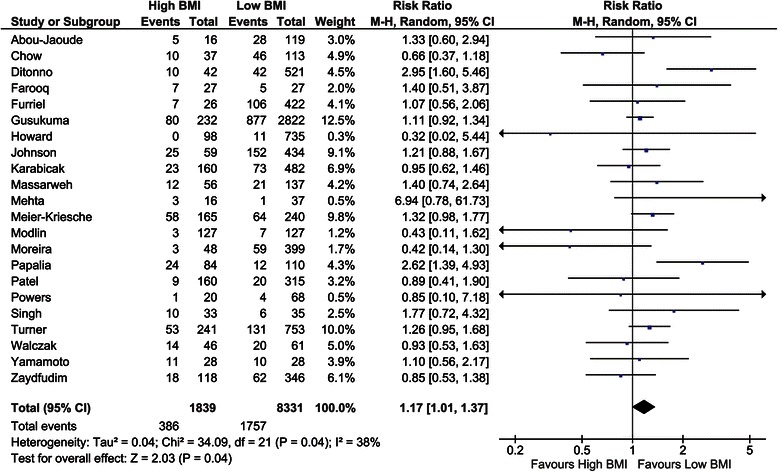
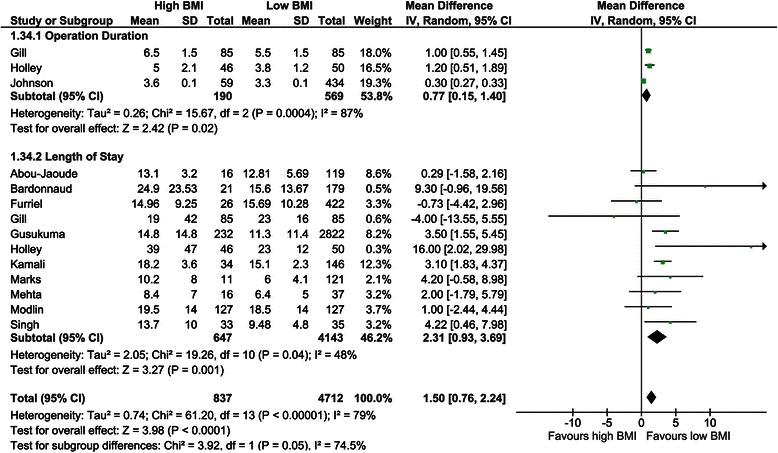
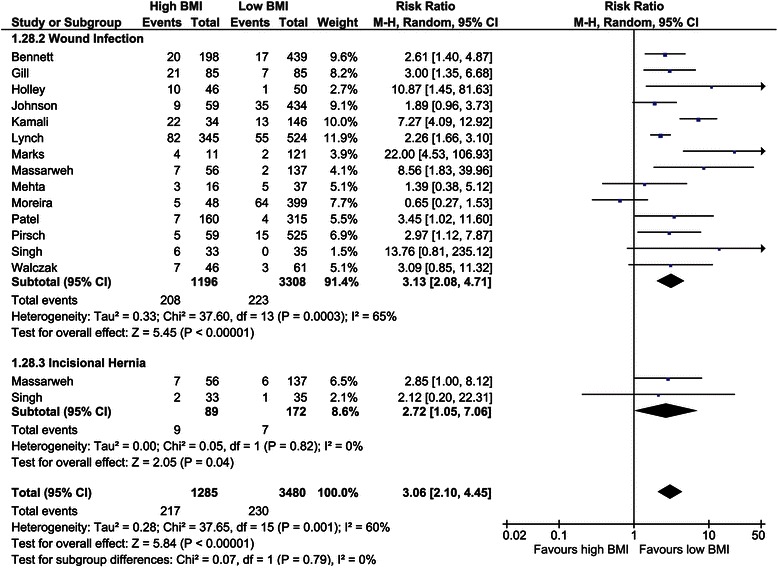
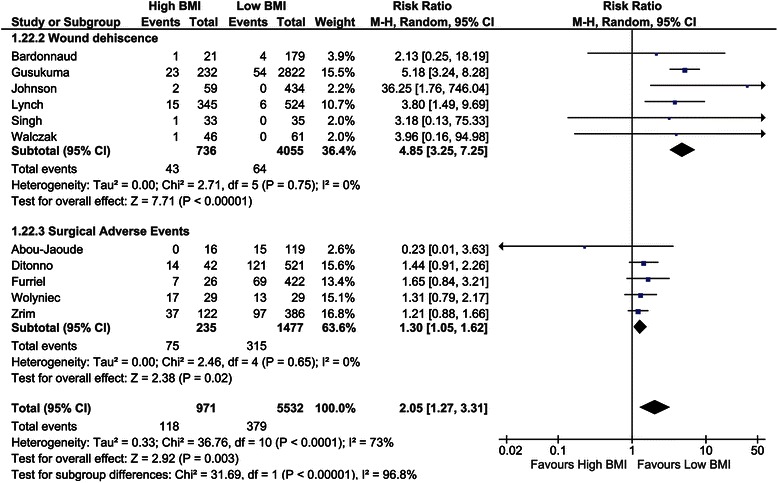
Results: After identifying 5,526 studies addressing this topic, 56 studies were included. We extracted data for 37 outcome measures (including data of more than 209,000 RT recipients), of which 26 could be meta-analysed. The following outcome measures demonstrated significant differences in favour of low BMI (<30) recipients: mortality (RR = 1.52), delayed graft function (RR = 1.52), acute rejection (RR = 1.17), 1-, 2-, and 3-year graft survival (RR = 0.97, 0.95, and 0.97), 1-, 2-, and 3-year patient survival (RR = 0.99, 0.99, and 0.99), wound infection and dehiscence (RR = 3.13 and 4.85), NODAT (RR = 2.24), length of hospital stay (2.31 days), operation duration (0.77 hours), hypertension (RR = 1.35), and incisional hernia (RR = 2.72). However, patient survival expressed in hazard ratios was in significant favour of high BMI recipients. Differences in other outcome parameters were not significant.
Conclusions: Several of the pooled outcome measurements show significant benefits for 'low' BMI (<30) recipients. Therefore, we postulate that ESRD patients with a BMI >30 preferably should lose weight prior to RT. If this cannot be achieved with common measures, in morbidly obese RT candidates, bariatric surgery could be considered.
Figures
References
-
- The Renal Association Assessment of the Potential Kidney Transplant Recipient. The Renal Association. 2011. http://www.renal.org/guidelines/modules/assessment-of-the-potential-kidn....
-
- Turner C, Nogueira J. The effect of obesity on allograft outcomes in a single-center cohort of living renal transplant recipients. Am J Transplant. 2007;7:464.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
