

Utility of adenosine deaminase (ADA), PCR & thoracoscopy in differentiating tuberculous & non-tuberculous pleural effusion complicating chronic kidney disease
- PMID: 25963491
- PMCID: PMC4442328
- DOI: 10.4103/0971-5916.156609
Utility of adenosine deaminase (ADA), PCR & thoracoscopy in differentiating tuberculous & non-tuberculous pleural effusion complicating chronic kidney disease
Abstract
Background & objectives: Pleural effusion is a common occurrence in patients with late-stage chronic kidney disease (CKD). In developing countries, many effusions remain undiagnosed after pleural fluid analysis (PFA) and patients are empirically treated with antitubercular therapy. The aim of this study was to evaluate the role of adenosine deaminase (ADA), nucleic acid amplification tests (NAAT) and medical thoracoscopy in distinguishing tubercular and non-tubercular aetiologies in exudative pleural effusions complicating CKD.
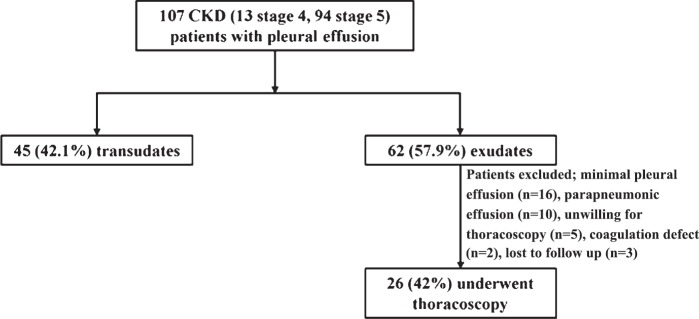
Methods: Consecutive stage 4 and 5 CKD patients with pleural effusions underwent PFA including ADA and PCR [65 kDa gene; multiplex (IS6110, protein antigen b, MPB64)]. Patients with exudative pleural effusion undiagnosed after PFA underwent medical thoracoscopy.
Results: All 107 patients underwent thoracocentesis with 45 and 62 patients diagnosed as transudative and exudative pleural effusions, respectively. Twenty six of the 62 patients underwent medical thoracoscopy. Tuberculous pleurisy was diagnosed in six while uraemic pleuritis was diagnosed in 20 subjects. The sensitivity and specificity of pleural fluid ADA, 65 kDa gene PCR, and multiplex PCR were 66.7 and 90 per cent, 100 and 50 per cent, and 100 and 100 per cent, respectively. Thoracoscopy was associated with five complications in three patients.
Interpretation & conclusions: Uraemia remains the most common cause of pleural effusion in CKD even in high TB prevalence country. Multiplex PCR and thoracoscopy are useful investigations in the diagnostic work-up of pleural effusions complicating CKD while the sensitivity and/or specificity of ADA and 65 kDa gene PCR is poor.
Figures
Comment in
-
Exudative pleural effusion in chronic kidney disease: An aetiological dilemma.Indian J Med Res. 2015 Mar;141(3):269-70. doi: 10.4103/0971-5916.156548. Indian J Med Res. 2015. PMID: 25963486 Free PMC article. No abstract available.
References
-
- Maher JF. Uremic pleuritis. Am J Kidney Dis. 1987;10:19–22. - PubMed
-
- Rashid-Farokhi F, Pourdowlat G, Nikoonia MR, Behzadnia N, Kahkouee S, Nassiri AA, et al. Uremic pleuritis in chronic hemodialysis patients. Hemodial Int. 2013;17:94–100. - PubMed
-
- McGrath EE, Anderson PB. Diagnostic tests for tuberculous pleural effusion. Eur J Clin Microbiol Infect Dis. 2010;29:1187–93. - PubMed
-
- Sahn SA, Huggins JT, San Jose ME, Alvarez-Dobano JM, Valdes L. Can tuberculous pleural effusions be diagnosed by pleural fluid analysis alone? Int J Tuberc Lung Dis. 2013;17:787–93. - PubMed
-
- Greco S, Girardi E, Masciangelo R, Capoccetta GB, Saltini C. Adenosine deaminase and interferon gamma measurements for the diagnosis of tuberculous pleurisy: a meta-analysis. Int J Tuberc Lung Dis. 2003;7:777–86. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials