

Evaluating the pharmacodynamic effect of antimalarial drugs in clinical trials by quantitative PCR
- PMID: 25963983
- PMCID: PMC4468738
- DOI: 10.1128/AAC.04942-14
Evaluating the pharmacodynamic effect of antimalarial drugs in clinical trials by quantitative PCR
Abstract
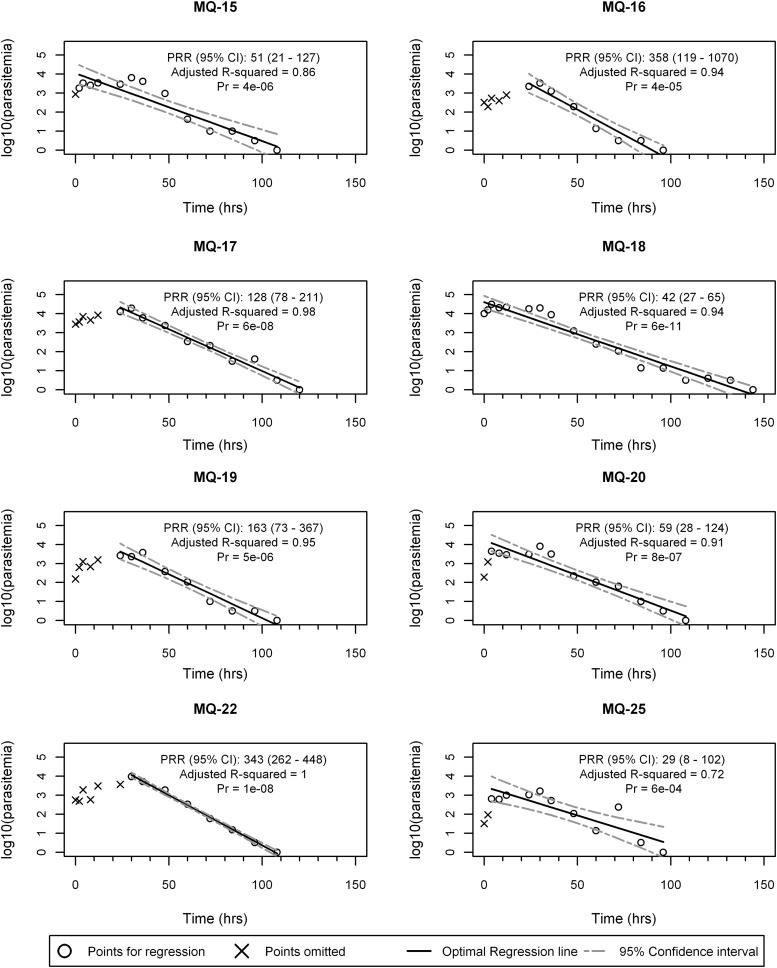
The ongoing development of new antimalarial drugs and the increasing use of controlled human malaria infection (CHMI) studies to investigate their activity in early-stage clinical trials require the development of methods to analyze their pharmacodynamic effect. This is especially so for studies where quantitative PCR (qPCR) is becoming the preferred method for assessing parasite clearance as the study endpoint. We report the development and validation of an analytic approach for qPCR-determined parasite clearance data. First, in a clinical trial with the licensed antimalarial combination sulfadoxine-pyrimethamine (S/P), qPCR data were collected from 12 subjects and used to determine qPCR replicate variability and to identify outliers. Then, an iterative analytic approach based on modeling the log-linear decay of parasitemia following drug treatment was developed to determine the parasite reduction ratio (PRR) and parasite clearance half-life, both measures of parasite clearance. This analytic approach was then validated with data from 8 subjects enrolled in a second study with the licensed antimalarial drug mefloquine. By this method, the PRR and parasite clearance half-lives for S/P and Mefloquine were determined to be 38,878 (95% confidence interval [95% CI], 17,396 to 86,889) at 3.15 (95% CI, 2.93 to 3.41) days and 157 (95% CI, 130 to 189) at 6.58 (95% CI, 6.35 to 6.83) days for the respective studies. No serious adverse events occurred in the two trials, and pharmacokinetic values were within expected ranges for sulfadoxine and pyrimethamine. The robust statistical method that we have developed to analyze qPCR-derived pharmacodynamic data from CHMI studies will facilitate the assessment of the activity of a range of experimental antimalarial drugs now entering clinical trials. (This trial was registered with the Australian New Zealand Clinical Trials Registry under registration numbers ACTRN12611001203943 and ACTRN12612000323820.).
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Dondorp AM, Fanello CI, Hendriksen IC, Gomes E, Seni A, Chhaganlal KD, Bojang K, Olaosebikan R, Anunobi N, Maitland K, Kivaya E, Agbenyega T, Nguah SB, Evans J, Gesase S, Kahabuka C, Mtove G, Nadjm B, Deen J, Mwanga-Amumpaire J, Nansumba M, Karema C, Umulisa N, Uwimana A, Mokuolu OA, Adedoyin OT, Johnson WB, Tshefu AK, Onyamboko MA, Sakulthaew T, Ngum WP, Silamut K, Stepniewska K, Woodrow CJ, Bethell D, Wills B, Oneko M, Peto TE, von Seidlein L, Day NP, White NJ. 2010. Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial. Lancet 376:1647–1657. doi:10.1016/S0140-6736(10)61924-1. - DOI - PMC - PubMed
-
- Amaratunga C, Sreng S, Suon S, Phelps ES, Stepniewska K, Lim P, Zhou C, Mao S, Anderson JM, Lindegardh N, Jiang H, Song J, Su XZ, White NJ, Dondorp AM, Anderson TJ, Fay MP, Mu J, Duong S, Fairhurst RM. 2012. Artemisinin-resistant Plasmodium falciparum in Pursat province, western Cambodia: a parasite clearance rate study. Lancet Infect Dis 12:851–858. doi:10.1016/S1473-3099(12)70181-0. - DOI - PMC - PubMed
-
- Ashley EA, Dhorda M, Fairhurst RM, Amaratunga C, Lim P, Suon S, Sreng S, Anderson JM, Mao S, Sam B, Sopha C, Chuor CM, Nguon C, Sovannaroth S, Pukrittayakamee S, Jittamala P, Chotivanich K, Chutasmit K, Suchatsoonthorn C, Runcharoen R, Hien TT, Thuy-Nhien NT, Thanh NV, Phu NH, Htut Y, Han KT, Aye KH, Mokuolu OA, Olaosebikan RR, Folaranmi OO, Mayxay M, Khanthavong M, Hongvanthong B, Newton PN, Onyamboko MA, Fanello CI, Tshefu AK, Mishra N, Valecha N, Phyo AP, Nosten F, Yi P, Tripura R, Borrmann S, Bashraheil M, Peshu J, Faiz MA, Ghose A, Hossain MA, Samad R, Rahman MR, Hasan MM, Islam A, Miotto O, Amato R, MacInnis B, Stalker J, Kwiatkowski DP, Bozdech Z, Jeeyapant A, Cheah PY, Sakulthaew T, Chalk J, Intharabut B, Silamut K, Lee SJ, Vihokhern B, Kunasol C, Imwong M, Tarning J, Taylor WJ, Yeung S, Woodrow CJ, Flegg JA, Das D, Smith J, Venkatesan M, Plowe CV, Stepniewska K, Guerin PJ, Dondorp AM, Day NP, White NJ, Tracking Resistance to Artemisinin Collaboration (TRAC). 2014. Spread of artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med 371:411–423. doi:10.1056/NEJMoa1314981. - DOI - PMC - PubMed
-
- Dondorp AM, Nosten F, Yi P, Das D, Phyo AP, Tarning J, Lwin KM, Ariey F, Hanpithakpong W, Lee SJ, Ringwald P, Silamut K, Imwong M, Chotivanich K, Lim P, Herdman T, An SS, Yeung S, Singhasivanon P, Day NP, Lindegardh N, Socheat D, White NJ. 2009. Artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med 361:455–467. doi:10.1056/NEJMoa0808859. - DOI - PMC - PubMed
-
- Phyo AP, Nkhoma S, Stepniewska K, Ashley EA, Nair S, McGready R, ler Moo C, Al-Saai S, Dondorp AM, Lwin KM, Singhasivanon P, Day NP, White NJ, Anderson TJ, Nosten F. 2012. Emergence of artemisinin-resistant malaria on the western border of Thailand: a longitudinal study. Lancet 379:1960–1966. doi:10.1016/S0140-6736(12)60484-X. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
