

Preoperative serum CA125: a useful marker for surgical management of endometrial cancer
- PMID: 25964114
- PMCID: PMC4438478
- DOI: 10.1186/s12885-015-1260-7
Preoperative serum CA125: a useful marker for surgical management of endometrial cancer
Abstract
Background: Surgery plays an important role in the management of endometrial cancer at all stages, particularly early clinical stage. There are still many unanswered questions regarding optimal surgical management of endometrial cancer, particularly regarding which patients should undergo lymphadenectomy. The aim of this study was to evaluate the role of preoperative cancer antigen 125 (CA125) serum levels for surgical management in endometrial cancer patients.
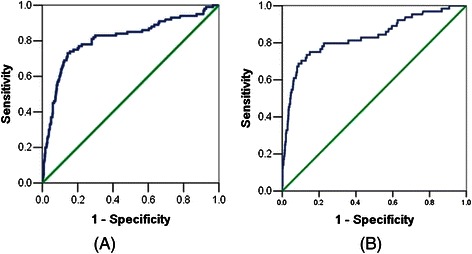
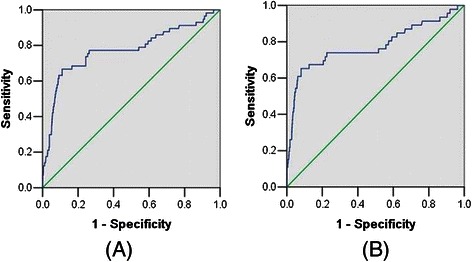
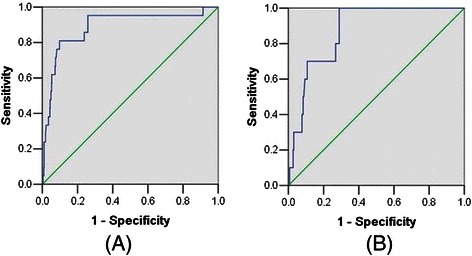
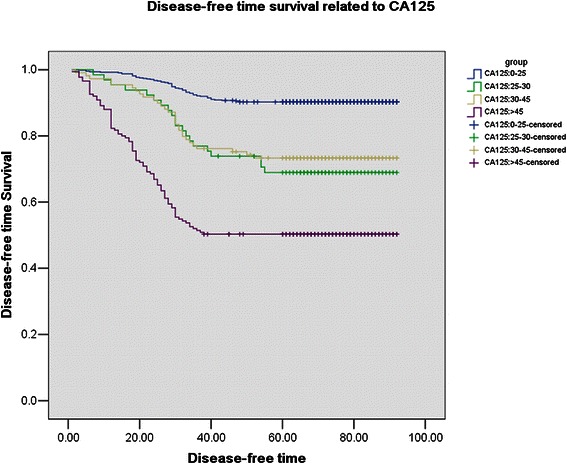
Methods: A total of 995 patients with endometrial cancer, according to inclusion criteria of a preoperative serum level of CA125, were selected. The association between clinicopathological factors and CA125 were analyzed. Receiver operating characteristic (ROC) curve was used to evaluate the role of preoperative serum CA125 in predicting lymph node metastasis, adnexal involement, cervical stromal invasion in all patients, especially patients with clinical stage I. Survival analyses were also performed according to the four groups of preoperative CA125 serum levels.
Results: Elevated CA125 level was significantly associated with all clinicopathological parameters, including age and menopause, but not histology type. ROC curve analysis results showed the CA125 serum level of 25 U/mL was the best cutoff to predict the lymph node metastasis. It was with 78% of sensitivity, 78% of specificity, 77.6% of false positive rate, 2.3% of false negative rate in all patients. In patients with clinical stage I, it was with 71.7% of sensitivity, 77.6% of specificity, 83.3% of false positive rate, 2.2% of false negative rate. The best cutoff to evaluate adnexal involement in patients with clinical stage I was 30U/ml, with 81% sensitivity, and 78.4% specificity. Survival analysis revealed CA125, FIGO stage, histology grade, and positive peritoneal cytology as independent prognostic factors of endometrial cancer.
Conclusion: Preoperative serum CA125 is an important predictor for patients with endometrial cancer and it should be taken into consideration when surgical management is determined, especially if a lymphadenectomy should be undertaken in patients with clinical stage I.
Figures
Similar articles
-
The prognostic role of preoperative serum CA125 levels in patients with advanced endometrial carcinoma.Cancer Biomark. 2017 Aug 23;20(2):135-141. doi: 10.3233/CBM-160529. Cancer Biomark. 2017. PMID: 28800309
-
Value of pre-operative serum CA125 level for prediction of prognosis in patients with endometrial cancer.Aust N Z J Obstet Gynaecol. 2011 Oct;51(5):397-402. doi: 10.1111/j.1479-828X.2011.01325.x. Epub 2011 Jun 9. Aust N Z J Obstet Gynaecol. 2011. PMID: 21806586
-
HE4 and CA125 levels in the preoperative assessment of endometrial cancer patients: a prospective multicenter study (ENDOMET).Acta Obstet Gynecol Scand. 2013 Nov;92(11):1313-22. doi: 10.1111/aogs.12235. Acta Obstet Gynecol Scand. 2013. PMID: 24032654
-
Diagnostic Accuracy of Clinical Biomarkers for Preoperative Prediction of Lymph Node Metastasis in Endometrial Carcinoma: A Systematic Review and Meta-Analysis.Oncologist. 2019 Sep;24(9):e880-e890. doi: 10.1634/theoncologist.2019-0117. Epub 2019 Jun 11. Oncologist. 2019. PMID: 31186375 Free PMC article.
-
HE4 tumor marker as a predictive factor for lymphatic metastasis in endometrial cancer.Int J Gynaecol Obstet. 2020 Jun;149(3):265-268. doi: 10.1002/ijgo.13140. Epub 2020 Apr 3. Int J Gynaecol Obstet. 2020. PMID: 32147821 Review.
Cited by
-
Factors associated with serum CA125 level in women without ovarian cancer in the United States: a population-based study.BMC Cancer. 2022 May 14;22(1):544. doi: 10.1186/s12885-022-09637-7. BMC Cancer. 2022. PMID: 35568827 Free PMC article.
-
Assessment of levels of the tumor markers HE4 and CA125 considering staging, grading and histological types of endometrial cancer.Prz Menopauzalny. 2016 Nov;15(3):133-137. doi: 10.5114/pm.2016.63059. Epub 2016 Nov 15. Prz Menopauzalny. 2016. PMID: 27980523 Free PMC article.
-
Controversies in the Management of Early-stage Serous Endometrial Cancer.In Vivo. 2021 Mar-Apr;35(2):671-680. doi: 10.21873/invivo.12307. In Vivo. 2021. PMID: 33622859 Free PMC article. Review.
-
What is the predictive value of preoperative CA 125 level on the survival rate of type 1 endometrial cancer?Turk J Med Sci. 2021 Feb 26;51(1):335-341. doi: 10.3906/sag-2005-331. Turk J Med Sci. 2021. PMID: 32979897 Free PMC article.
-
Oncofetal reprogramming in tumour development and progression.Nat Rev Cancer. 2022 Oct;22(10):593-602. doi: 10.1038/s41568-022-00497-8. Epub 2022 Aug 23. Nat Rev Cancer. 2022. PMID: 35999292 Review.
References
-
- Beesley VL, Rowlands IJ, Hayes SC, Janda M, O’Rourke P, Marquart L, et al. Incidence, risk factors and estimates of a woman’s risk of developing secondary lower limb lymphedema and lymphedema-specific supportive care needs in women treated for endometrial cancer. Gynecol Oncol. 2015;136:87–93. doi: 10.1016/j.ygyno.2014.11.006. - DOI - PubMed
-
- Salani R, Preston MM, Hade EM, Johns J, Fowler JM, Paskett EP, et al. Swelling among women who need education about leg lymphedema: a descriptive study of lymphedema in women undergoing surgery for endometrial cancer. Int J Gynecol Cancer. 2014;24:1507–12. doi: 10.1097/IGC.0000000000000226. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
