

Risk Algorithm Using Serial Biomarker Measurements Doubles the Number of Screen-Detected Cancers Compared With a Single-Threshold Rule in the United Kingdom Collaborative Trial of Ovarian Cancer Screening
- PMID: 25964255
- PMCID: PMC4463475
- DOI: 10.1200/JCO.2014.59.4945
Risk Algorithm Using Serial Biomarker Measurements Doubles the Number of Screen-Detected Cancers Compared With a Single-Threshold Rule in the United Kingdom Collaborative Trial of Ovarian Cancer Screening
Abstract
Purpose: Cancer screening strategies have commonly adopted single-biomarker thresholds to identify abnormality. We investigated the impact of serial biomarker change interpreted through a risk algorithm on cancer detection rates.
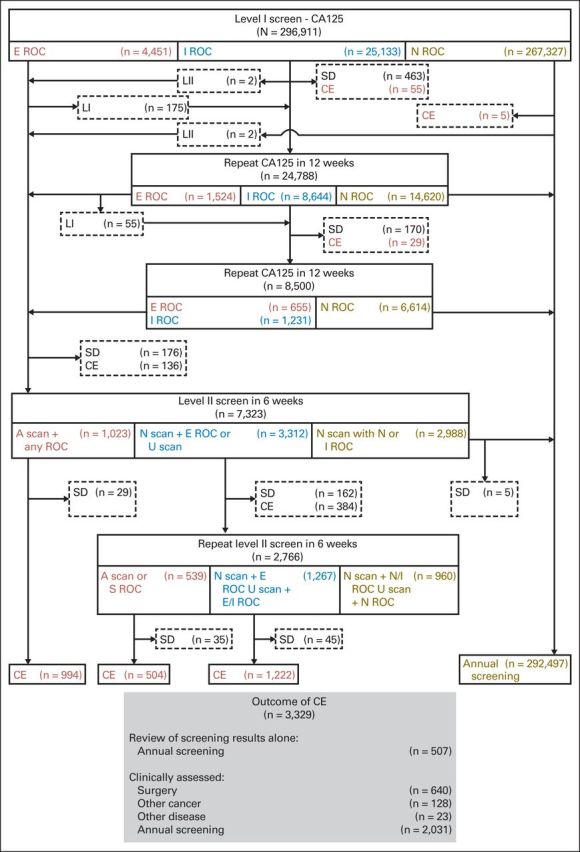
Patients and methods: In the United Kingdom Collaborative Trial of Ovarian Cancer Screening, 46,237 women, age 50 years or older underwent incidence screening by using the multimodal strategy (MMS) in which annual serum cancer antigen 125 (CA-125) was interpreted with the risk of ovarian cancer algorithm (ROCA). Women were triaged by the ROCA: normal risk, returned to annual screening; intermediate risk, repeat CA-125; and elevated risk, repeat CA-125 and transvaginal ultrasound. Women with persistently increased risk were clinically evaluated. All participants were followed through national cancer and/or death registries. Performance characteristics of a single-threshold rule and the ROCA were compared by using receiver operating characteristic curves.
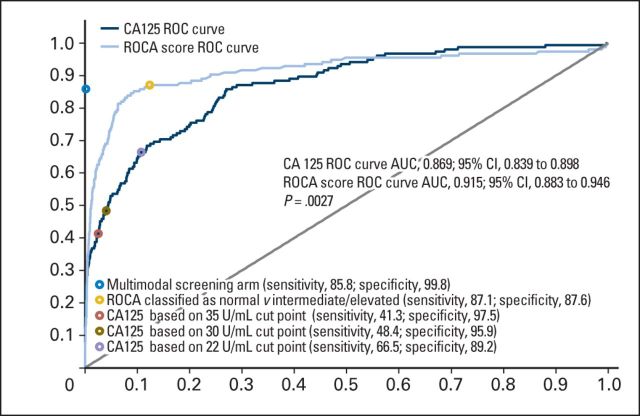
Results: After 296,911 women-years of annual incidence screening, 640 women underwent surgery. Of those, 133 had primary invasive epithelial ovarian or tubal cancers (iEOCs). In all, 22 interval iEOCs occurred within 1 year of screening, of which one was detected by ROCA but was managed conservatively after clinical assessment. The sensitivity and specificity of MMS for detection of iEOCs were 85.8% (95% CI, 79.3% to 90.9%) and 99.8% (95% CI, 99.8% to 99.8%), respectively, with 4.8 surgeries per iEOC. ROCA alone detected 87.1% (135 of 155) of the iEOCs. Using fixed CA-125 cutoffs at the last annual screen of more than 35, more than 30, and more than 22 U/mL would have identified 41.3% (64 of 155), 48.4% (75 of 155), and 66.5% (103 of 155), respectively. The area under the curve for ROCA (0.915) was significantly (P = .0027) higher than that for a single-threshold rule (0.869).
Conclusion: Screening by using ROCA doubled the number of screen-detected iEOCs compared with a fixed cutoff. In the context of cancer screening, reliance on predefined single-threshold rules may result in biomarkers of value being discarded.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures

Comment in
-
Change in blood protein detects more ovarian cancers than fixed threshold, study finds.BMJ. 2015 May 4;350:h2367. doi: 10.1136/bmj.h2367. BMJ. 2015. PMID: 25943947 No abstract available.
-
Gynaecological cancer: Biomarker potential of CA-125 enhanced.Nat Rev Clin Oncol. 2015 Aug;12(8):437. doi: 10.1038/nrclinonc.2015.95. Epub 2015 May 26. Nat Rev Clin Oncol. 2015. PMID: 26011486 No abstract available.
-
Definition of Specificity in a Screening Trial.J Clin Oncol. 2016 Jan 10;34(2):198. doi: 10.1200/JCO.2015.62.9253. Epub 2015 Nov 16. J Clin Oncol. 2016. PMID: 26573070 No abstract available.
-
Ovarian Cancer Early Detection Needs Better Imaging, Not Better Algorithms or Biomarkers.J Clin Oncol. 2016 Jan 10;34(2):199-200. doi: 10.1200/JCO.2015.63.7843. Epub 2015 Nov 16. J Clin Oncol. 2016. PMID: 26573076 No abstract available.
-
Preventing Ovarian Cancer.J Clin Oncol. 2016 Jan 10;34(2):198-9. doi: 10.1200/JCO.2015.62.9519. Epub 2015 Nov 16. J Clin Oncol. 2016. PMID: 26573077 No abstract available.
-
Reply to P.F. Pinsky, C.P. Crum, and M.W. McIntosh et al.J Clin Oncol. 2016 Jan 10;34(2):201-2. doi: 10.1200/JCO.2015.64.1365. Epub 2015 Nov 16. J Clin Oncol. 2016. PMID: 26573079 No abstract available.
-
Ovarian Cancer Screening There May Be Light at the End of the Tunnel?Int J Gynecol Cancer. 2016 May;26(4):608-9. doi: 10.1097/IGC.0000000000000706. Int J Gynecol Cancer. 2016. PMID: 27101522 No abstract available.
References
-
- van den Bergh RC, Roemeling S, Roobol MJ, et al. Prostate-specific antigen kinetics in clinical decision-making during active surveillance for early prostate cancer: A review. Eur Urol. 2008;54:505–516. - PubMed
-
- Loeb S, Carter HB. Point: Impact of prostate-specific antigen velocity on management decisions and recommendations. J Natl Compr Canc Netw. 2013;11:281–285. - PubMed
-
- Pinsky PF, Zhu C, Skates SJ, et al. Potential effect of the risk of ovarian cancer algorithm (ROCA) on the mortality outcome of the Prostate, Lung, Colorectal and Ovarian (PLCO) trial. Int J Cancer. 2013;132:2127–2133. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
