

How I treat hypereosinophilic syndromes
- PMID: 25964669
- PMCID: PMC4551360
- DOI: 10.1182/blood-2014-11-551614
How I treat hypereosinophilic syndromes
Abstract
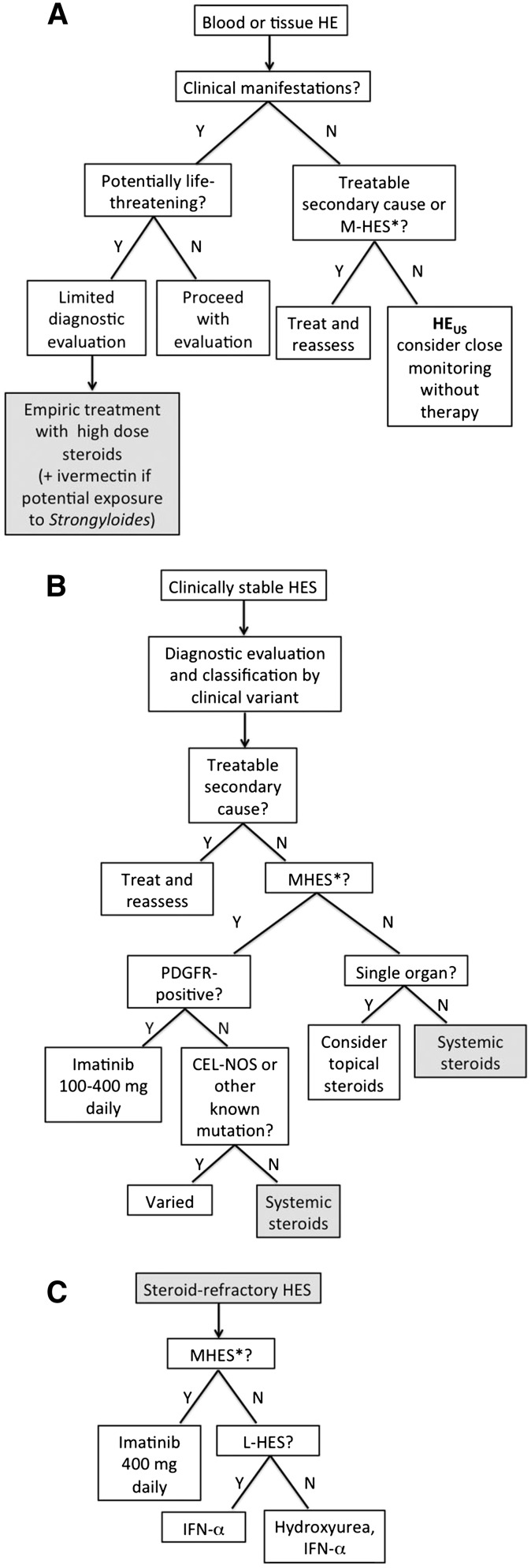
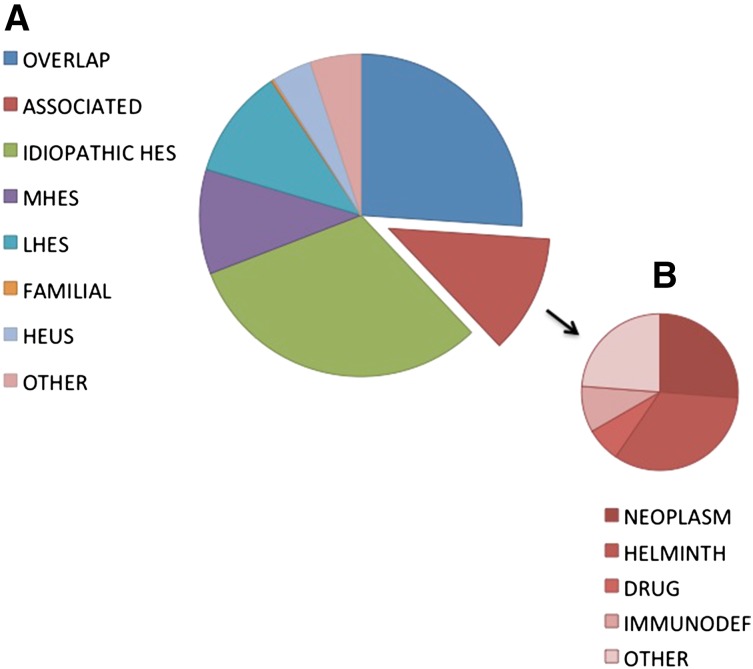
Hypereosinophilic syndromes (HESs) are a group of rare disorders characterized by peripheral blood eosinophilia of 1.5 × 10(9)/L or higher and evidence of end organ manifestations attributable to the eosinophilia and not otherwise explained in the clinical setting. HESs are pleomorphic in clinical presentation and can be idiopathic or associated with a variety of underlying conditions, including allergic, rheumatologic, infectious, and neoplastic disorders. Moreover, the etiology of the eosinophilia in HESs can be primary (myeloid), secondary (lymphocyte-driven), or unknown. Although corticosteroids remain the first-line therapy for most forms of HESs, the availability of an increasing number of novel therapeutic agents, including tyrosine kinase inhibitors and monoclonal antibodies, has necessarily altered the approach to treatment of HESs. This review presents an updated treatment-based approach to the classification of patients with presumed HES and discusses the roles of conventional and novel agents in the management of these patients.
Figures
References
-
- Andersen CL, Siersma VD, Hasselbalch HC, et al. Eosinophilia in routine blood samples and the subsequent risk of hematological malignancies and death. Am J Hematol. 2013;88(10):843–847. - PubMed
-
- Schulte C, Krebs B, Jelinek T, Nothdurft HD, von Sonnenburg F, Löscher T. Diagnostic significance of blood eosinophilia in returning travelers. Clin Infect Dis. 2002;34(3):407–411. - PubMed
-
- Hardy WR, Anderson RE. The hypereosinophilic syndromes. Ann Intern Med. 1968;68(6):1220–1229. - PubMed
-
- Swerdlow S, Campo E, Harris NL, editors. WHO Classification of Tumours of Hematopoietic and Lymphoid Tissue. Geneva, Switzerland: World Health Organization; 2008.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
