

Impact of antiretroviral therapy on lipid metabolism of human immunodeficiency virus-infected patients: Old and new drugs
- PMID: 25964872
- PMCID: PMC4419122
- DOI: 10.5501/wjv.v4.i2.56
Impact of antiretroviral therapy on lipid metabolism of human immunodeficiency virus-infected patients: Old and new drugs
Abstract
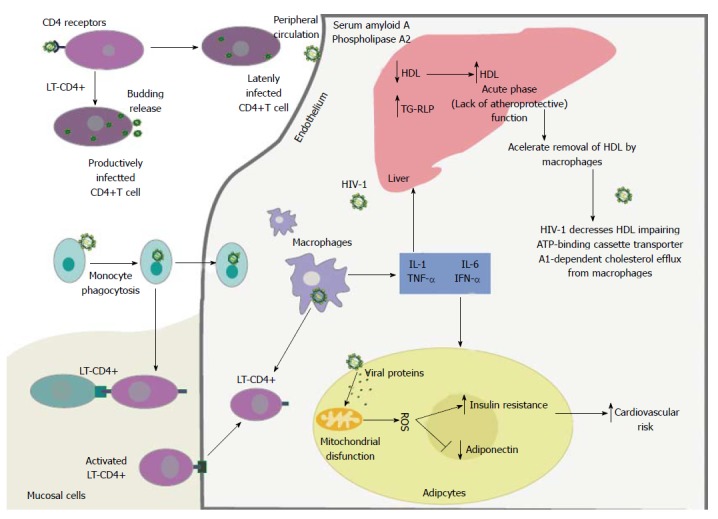
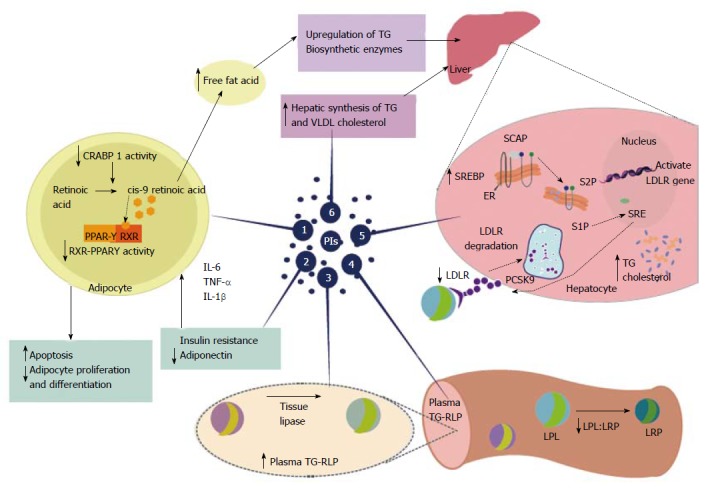
For human immunodeficiency virus (HIV)-infected patients, the 1990s were marked by the introduction of highly active antiretroviral therapy (HAART) representing a new perspective of life for these patients. The use of HAART was shown to effectively suppress the replication of HIV-1 and dramatically reduce mortality and morbidity, which led to a better and longer quality of life for HIV-1-infected patients. Apart from the substantial benefits that result from the use of various HAART regimens, laboratory and clinical experience has shown that HAART can induce severe and considerable adverse effects related to metabolic complications of lipid metabolism, characterized by signs of lipodystrophy, insulin resistance, central adiposity, dyslipidemia, increased risk of cardiovascular disease and even an increased risk of atherosclerosis. New drugs are being studied, new therapeutic strategies are being implemented, and the use of statins, fibrates, and inhibitors of intestinal cholesterol absorption have been effective alternatives. Changes in diet and lifestyle have also shown satisfactory results.
Keywords: Atherosclerosis; Diet; Dyslipidemia; Fibrates; Highly active antiretroviral therapy; Human immunodeficiency virus-1 infection; Lifestyle; Lipodystrophy; Protease inhibitors; Statins.
Figures
References
-
- Passaes CP, Sáez-Cirión A. HIV cure research: advances and prospects. Virology. 2014;454-455:340–352. - PubMed
-
- Calvo KR, Daar ES. Antiretroviral therapy: treatment-experienced individuals. Infect Dis Clin North Am. 2014;28:439–456. - PubMed
-
- Sobieszczyk ME, Talley AK, Wilkin T, Hammer SM. Advances in antiretroviral therapy. Top HIV Med. 2005;13:24–44. - PubMed
-
- Rigourd M, Lanchy JM, Le Grice SF, Ehresmann B, Ehresmann C, Marquet R. Inhibition of the initiation of HIV-1 reverse transcription by 3’-azido-3’-deoxythymidine. Comparison with elongation. J Biol Chem. 2000;275:26944–26951. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
