

Circulating Angiogenic Factors and the Risk of Adverse Outcomes among Haitian Women with Preeclampsia
- PMID: 25965397
- PMCID: PMC4428697
- DOI: 10.1371/journal.pone.0126815
Circulating Angiogenic Factors and the Risk of Adverse Outcomes among Haitian Women with Preeclampsia
Abstract
Objective: Angiogenic factors are strongly associated with adverse maternal and fetal outcomes among women with preterm preeclampsia (PE) in developed countries. We evaluated the role of angiogenic factors and their relationship to adverse outcomes among Haitian women with PE.
Material and methods: We measured plasma antiangiogenic soluble fms-like tyrosine kinase 1 (sFlt1) and proangiogenic placental growth factor (PlGF) levels in women with PE (n=35) compared to controls with no hypertensive disorders (NHD) (n=43) among subjects with singleton pregnancies that delivered at Hospital Albert Schweitzer (HAS) in Haiti. We divided the preeclamptic women into two groups, early onset (≤ 34 weeks) and late onset (>34 weeks) and examined relationships between sFlt1/PlGF ratios on admission and adverse outcomes (abruption, respiratory complications, stroke, renal insufficiency, eclampsia, maternal death, birth weight <2500 grams, or fetal/neonatal death) in women with PE subgroups as compared to NHD groups separated by week of admission. Data are presented as median (25th-75th centile), n (%), and proportions.
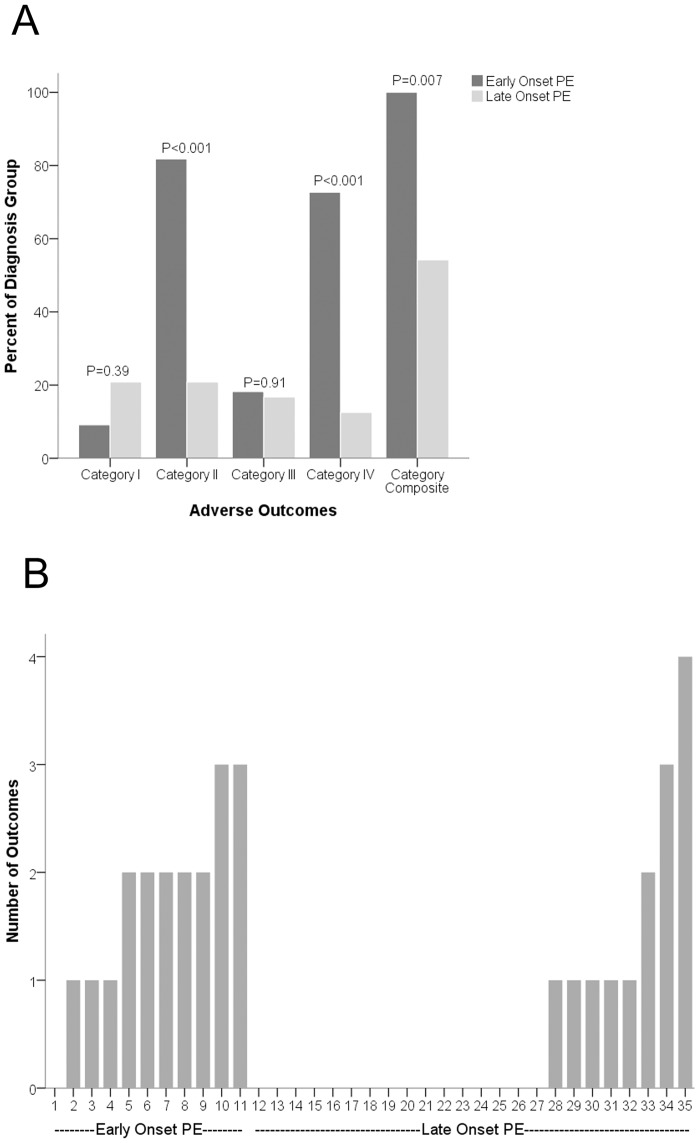
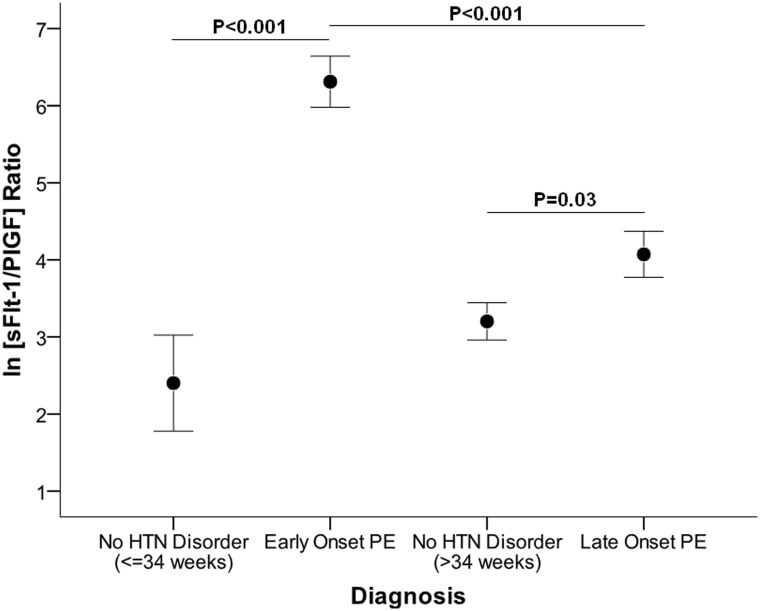
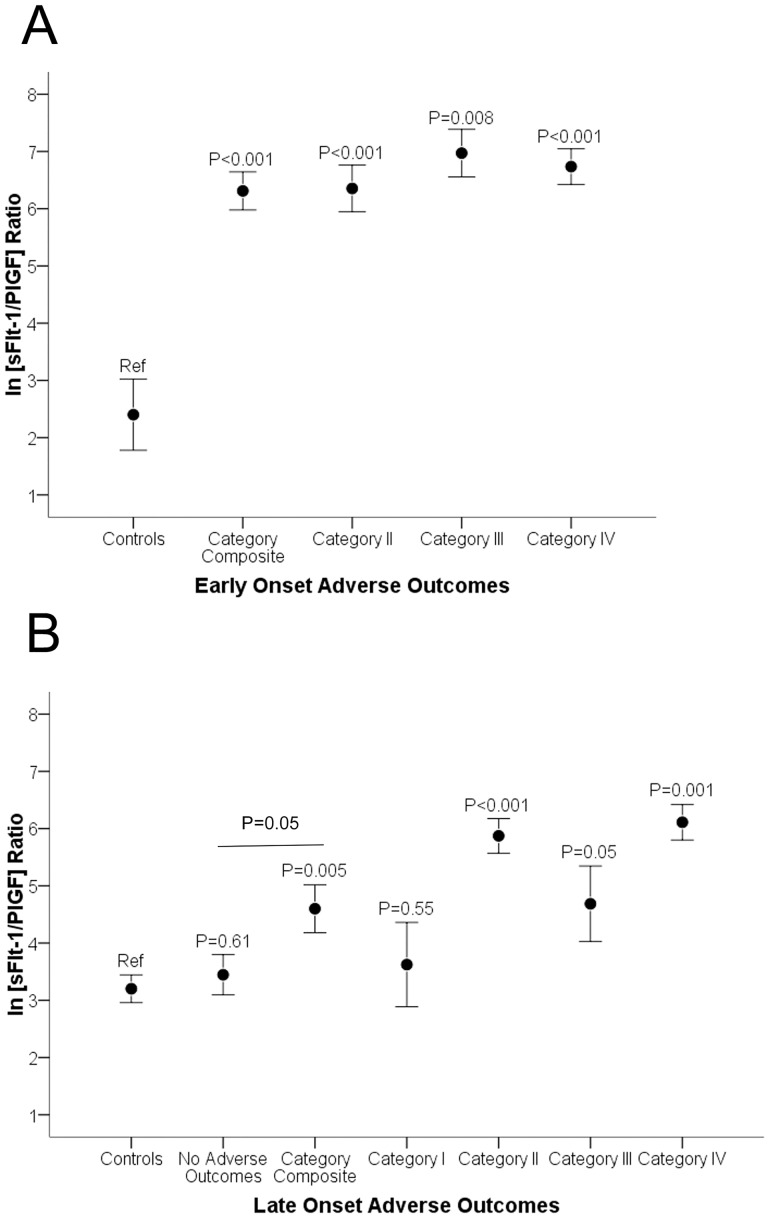
Results: Among patients with PE, most (24/35) were admitted at term. Adverse outcome rates in PE were much higher among the early onset group compared to the late onset group (100.0% vs. 54.2%, P=0.007). Plasma angiogenic factors were dramatically altered in both subtypes of PE. Angiogenic factors also correlated with adverse outcomes in both subtypes of PE. The median sFlt1/PlGF ratios for subjects with early onset PE with any adverse outcome vs. NHD <=34 weeks with no adverse outcome were 703.1 (146.6, 1614.9) and 9.6 (3.5, 58.6); P<0.001). Among late onset group the median sFlt1/PlGF ratio for women with any adverse outcome was 130.7 (56.1, 242.6) versus 22.4 (10.2, 58.7; P=0.005) in NHD >34 weeks with no adverse outcome.
Conclusion: PE-related adverse outcomes are common in women in Haiti and are associated with profound angiogenic imbalance regardless of gestational age at presentation.
Conflict of interest statement
Figures
References
-
- Organization WH. World Health Report Make every mother and child count. Geneva: 2005.
-
- ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. Obstet Gynecol. 2002;99(1):159–67. - PubMed
-
- Morisaki N, Togoobaatar G, Vogel JP, Souza JP, Rowland Hogue CJ, Jayaratne K, et al. Risk factors for spontaneous and provider-initiated preterm delivery in high and low Human Development Index countries: a secondary analysis of the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG. 2014;121 Suppl 1:101–9. 10.1111/1471-0528.12631 - DOI - PubMed
-
- Firoz T, Sanghvi H, Merialdi M, von Dadelszen P. Pre-eclampsia in low and middle income countries. Best practice & research Clinical obstetrics & gynaecology. 2011;25(4):537–48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
