

Cost comparison of transcatheter and operative closures of ostium secundum atrial septal defects
- PMID: 25965721
- PMCID: PMC4429255
- DOI: 10.1016/j.ahj.2015.02.010
Cost comparison of transcatheter and operative closures of ostium secundum atrial septal defects
Abstract
Background: Clinical outcomes for transcatheter and operative closures of atrial septal defects (ASDs) are similar. Economic cost for each method has not been well described.
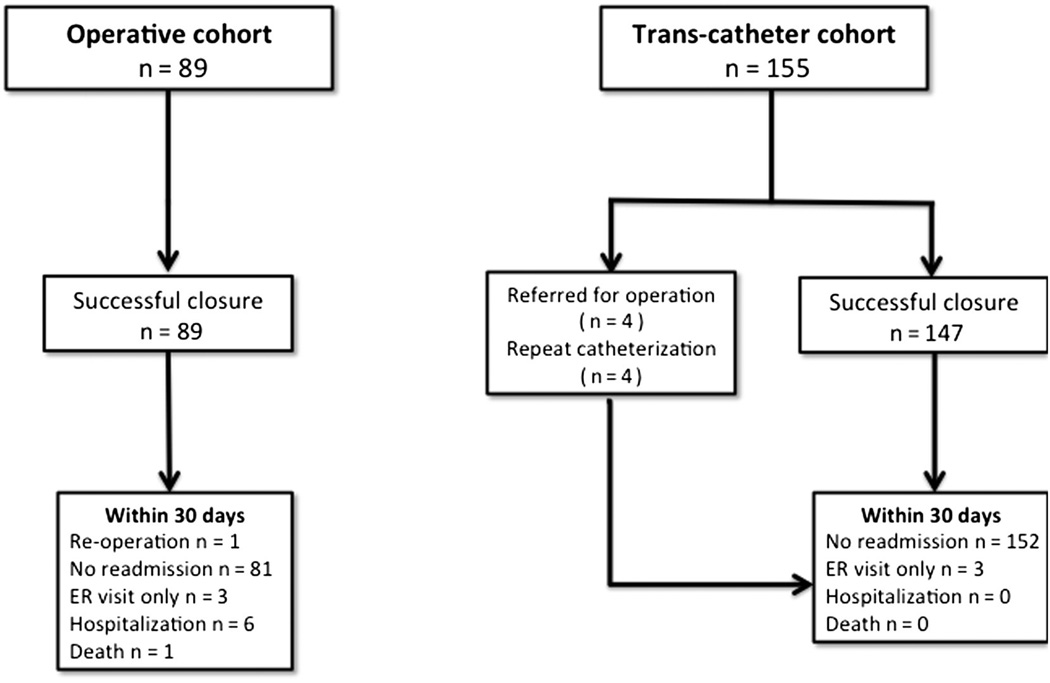
Methods: A single-center retrospective cohort study of children and adults<30 years of age undergoing closure for single secundum ASD from January 1, 2007, to April 1, 2012, was performed to measure differences in inflation-adjusted cost of operative and transcatheter closures of ASD. A propensity score weight-adjusted multivariate regression model was used in an intention-to-treat analysis. Costs for reintervention and crossover admissions were included in primary analysis.
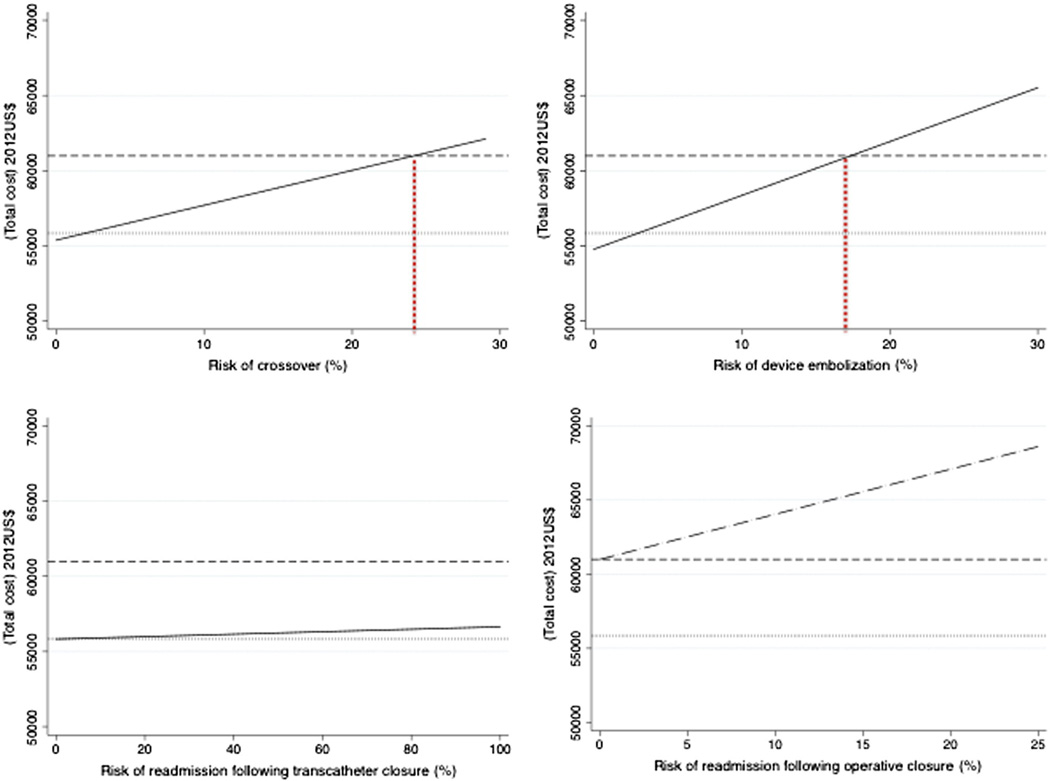
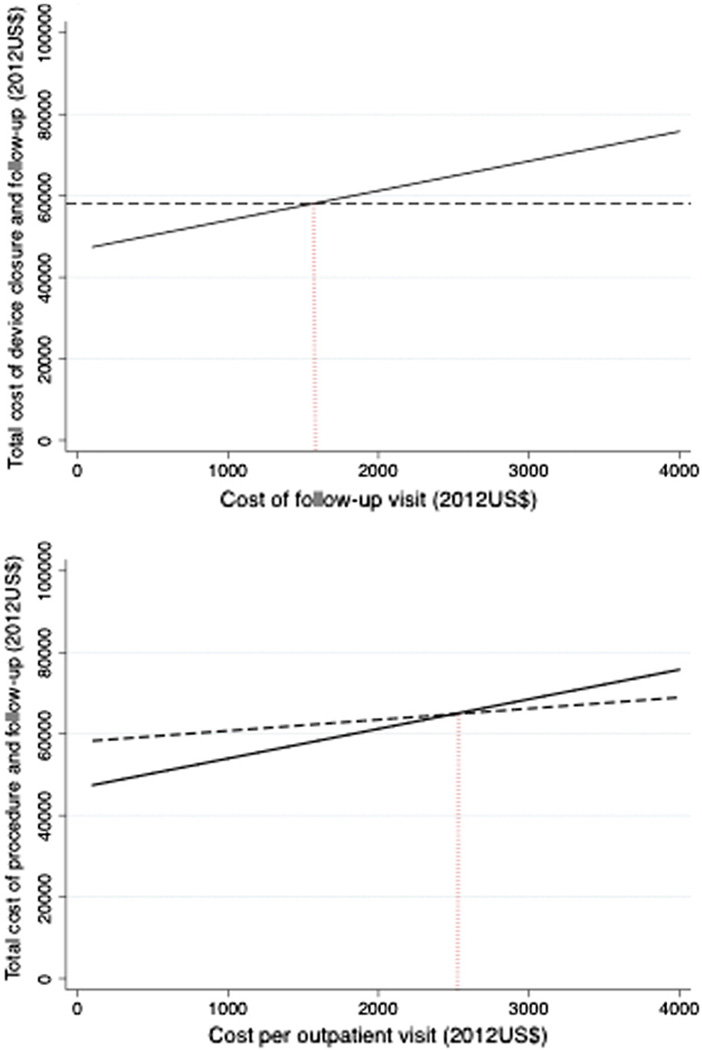
Results: A total of 244 subjects were included in the study (64% transcatheter and 36% operative), of which 2% (n = 5) were ≥18 years. Crossover rate from transcatheter to operative group was 3%. Risk of reintervention (P = .66) and 30-day mortality (P = .37) were not significantly different. In a multivariate model, adjusted cost of operative closure was 2012 US $60,992 versus 2012 US $55,841 for transcatheter closure (P < .001). Components of total cost favoring transcatheter closure were length of stay, medications, and follow-up radiologic and laboratory testing, overcoming higher costs of procedure and echocardiography. Professional costs did not differ. The rate of 30-day readmission was greater in the operative cohort, further increasing the cost advantage of transcatheter closure. Sensitivity analyses demonstrated that costs of follow-up visits influenced relative cost but that device closure remained favorable over a broad range of crossover and reintervention rates.
Conclusion: For single secundum ASD, cost comparison analysis favors transcatheter closure over the short term. The cost of follow-up regimens influences the cost advantage of transcatheter closure.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Transcatheter Versus Surgical Closure of Atrial Septal Defects in Children: A Value Comparison.JACC Cardiovasc Interv. 2016 Jan 11;9(1):79-86. doi: 10.1016/j.jcin.2015.09.028. JACC Cardiovasc Interv. 2016. PMID: 26762915
-
Clinical outcomes and costs of Amplatzer transcatheter closure as compared with surgical closure of ostium secundum atrial septal defects.Med Sci Monit. 2002 Dec;8(12):CR787-91. Med Sci Monit. 2002. PMID: 12503036
-
Long-term cost-effectiveness of transcatheter versus surgical closure of secundum atrial septal defect in adults.Int J Cardiol. 2014 Mar 1;172(1):109-14. doi: 10.1016/j.ijcard.2013.12.144. Epub 2014 Jan 8. Int J Cardiol. 2014. PMID: 24485223
-
Complications and Efficacies of Surgical Versus Transcatheter Closure for Pediatric Ostium Secundum Atrial Septal Defect: A Meta-Analysis.J Endovasc Ther. 2024 Apr 10:15266028241245599. doi: 10.1177/15266028241245599. Online ahead of print. J Endovasc Ther. 2024. PMID: 38597284 Review.
-
Atrial fibrillation following transcatheter atrial septal defect closure: a systematic review and meta-analysis.Heart. 2022 Jul 13;108(15):1216-1224. doi: 10.1136/heartjnl-2021-319794. Heart. 2022. PMID: 34675040
Cited by
-
Cost comparison of Transcatheter and Operative Pulmonary Valve Replacement (from the Pediatric Health Information Systems Database).Am J Cardiol. 2016 Jan 1;117(1):121-6. doi: 10.1016/j.amjcard.2015.10.011. Epub 2015 Oct 17. Am J Cardiol. 2016. PMID: 26552510 Free PMC article.
-
Comparison of Management Strategies for Neonates With Symptomatic Tetralogy of Fallot.J Am Coll Cardiol. 2021 Mar 2;77(8):1093-1106. doi: 10.1016/j.jacc.2020.12.048. J Am Coll Cardiol. 2021. PMID: 33632484 Free PMC article.
-
Increasing propensity to pursue operative closure of atrial septal defects following changes in the instructions for use of the Amplatzer Septal Occluder device: An observational study using data from the Pediatric Health Information Systems database.Am Heart J. 2017 Oct;192:85-97. doi: 10.1016/j.ahj.2017.07.012. Epub 2017 Jul 19. Am Heart J. 2017. PMID: 28938967 Free PMC article.
-
Outcomes of Operator-Directed Sedation and Anesthesiologist Care in the Pediatric/Congenital Catheterization Laboratory: A Study Utilizing Data From the IMPACT Registry.JACC Cardiovasc Interv. 2021 Feb 22;14(4):401-413. doi: 10.1016/j.jcin.2020.10.054. JACC Cardiovasc Interv. 2021. PMID: 33602437 Free PMC article.
-
Percutaneous atrial septal defect closure in limited-resource setting: a decade-long experience from Ethiopia.Front Cardiovasc Med. 2025 Feb 18;12:1550693. doi: 10.3389/fcvm.2025.1550693. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40041170 Free PMC article.
References
-
- King TD, Thompson SL, Steiner C, et al. Secundum atrial septal defect. Nonoperative closure during cardiac catheterization. JAMA. 1976;235(23):2506–2509. - PubMed
-
- Butera G, Biondi-Zoccai G, Sangiorgi G, et al. Percutaneous versus surgical closure of secundum atrial septal defects: a systematic review and meta-analysis of currently available clinical evidence. EuroIntervention. 2011;7(3):377–385. - PubMed
-
- Kutty S, Abu Hazeem A, Brown K, et al. AJC. 9. Vol. 109. Elsevier Inc.; 2012. Long-term (5- to 20-year) outcomes after transcatheter or surgical treatment of hemodynamically significant isolated secundum atrial septal defect; pp. 1348–1352. - PubMed
-
- Baker SS, O'Laughlin MP, Jollis JG, et al. Cost implications of closure of atrial septal defect. Catheter Cardiovasc Interv. 2001;55(1):83–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
