

Multiple clinical episodes of Plasmodium falciparum malaria in a low transmission intensity setting: exposure versus immunity
- PMID: 25967134
- PMCID: PMC4445794
- DOI: 10.1186/s12916-015-0354-z
Multiple clinical episodes of Plasmodium falciparum malaria in a low transmission intensity setting: exposure versus immunity
Abstract
Background: Epidemiological studies indicate that some children experience many more episodes of clinical malaria than their age mates in a given location. Whether this is as a result of the micro-heterogeneity of malaria transmission with some children effectively getting more exposure to infectious mosquitoes than others, or reflects a failure in the acquisition of immunity needs to be elucidated. Here, we investigated the determinants of increased susceptibility to clinical malaria by comparing the intensity of exposure to Plasmodium falciparum and the acquisition of immunity in children at the extreme ends of the over-dispersed distribution of the incidence of clinical malaria.
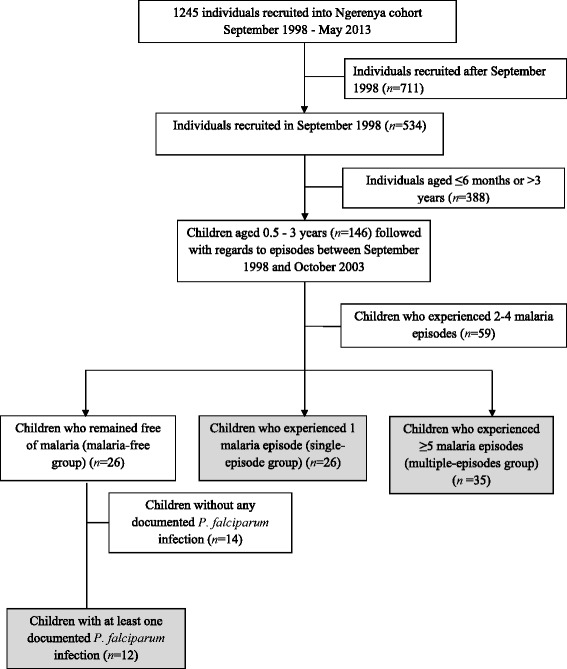
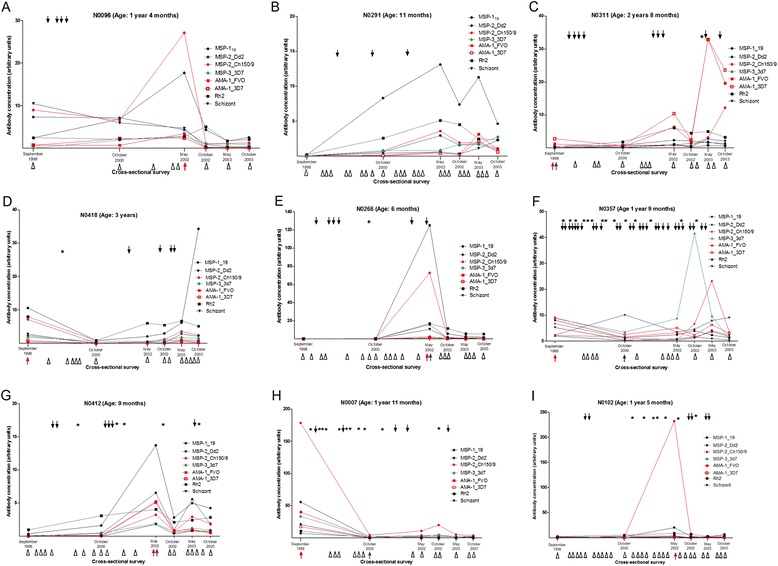
Methods: The study was nested within a larger cohort in an area where the intensity of malaria transmission was low. We identified children who over a five-year period experienced 5 to 16 clinical malaria episodes (children at the tail-end of the over-dispersed distribution, n = 35), remained malaria-free (n = 12) or had a single episode (n = 26). We quantified antibodies against seven Plasmodium falciparum merozoite antigens in plasma obtained at six cross-sectional surveys spanning these five years. We analyzed the antibody responses to identify temporal dynamics that associate with disease susceptibility.
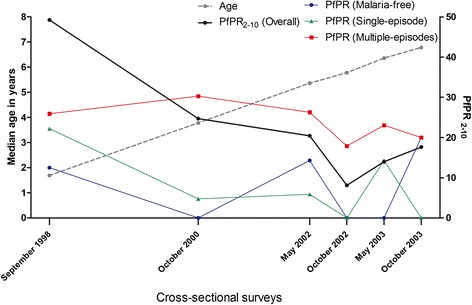
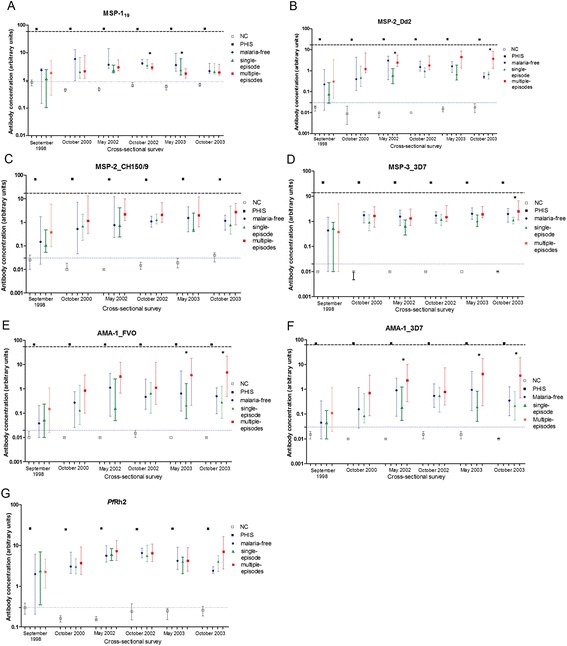
Results: Children experiencing multiple episodes of malaria were more likely to be parasite positive by microscopy at cross-sectional surveys (X (2) test for trend 14.72 P = 0.001) and had a significantly higher malaria exposure index, than those in the malaria-free or single episode groups (Kruskal-Wallis test P = 0.009). In contrast, the five-year temporal dynamics of anti-merozoite antibodies were similar in the three groups. Importantly in all groups, antibody levels were below the threshold concentrations previously observed to be correlated with protective immunity.
Conclusions: We conclude that in the context of a low malaria transmission setting, susceptibility to clinical malaria is not accounted for by anti-merozoite antibodies but appears to be a consequence of increased parasite exposure. We hypothesize that intensive exposure is a prerequisite for protective antibody concentrations, while little to modest exposure may manifest as multiple clinical infections with low levels of antibodies. These findings have implications for interventions that effectively lower malaria transmission intensity.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
