

TLR9-Targeted STAT3 Silencing Abrogates Immunosuppressive Activity of Myeloid-Derived Suppressor Cells from Prostate Cancer Patients
- PMID: 25967142
- PMCID: PMC4537814
- DOI: 10.1158/1078-0432.CCR-14-3145
TLR9-Targeted STAT3 Silencing Abrogates Immunosuppressive Activity of Myeloid-Derived Suppressor Cells from Prostate Cancer Patients
Abstract
Purpose: Recent advances in immunotherapy of advanced human cancers underscored the need to address and eliminate tumor immune evasion. The myeloid-derived suppressor cells (MDSC) are important inhibitors of T-cell responses in solid tumors, such as prostate cancers. However, targeting MDSCs proved challenging due to their phenotypic heterogeneity.
Experimental design: Myeloid cell populations were evaluated using flow cytometry on blood samples, functional assays, and immunohistochemical/immunofluorescent stainings on specimens from healthy subjects, localized and metastatic castration-resistant prostate cancer patients.
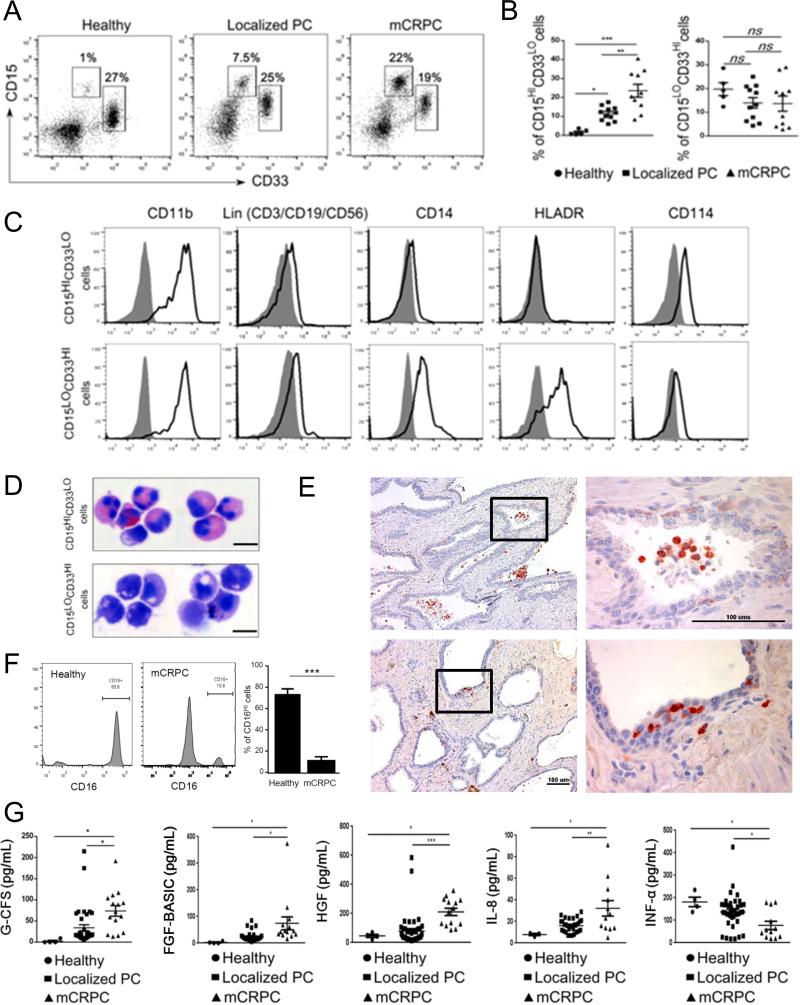
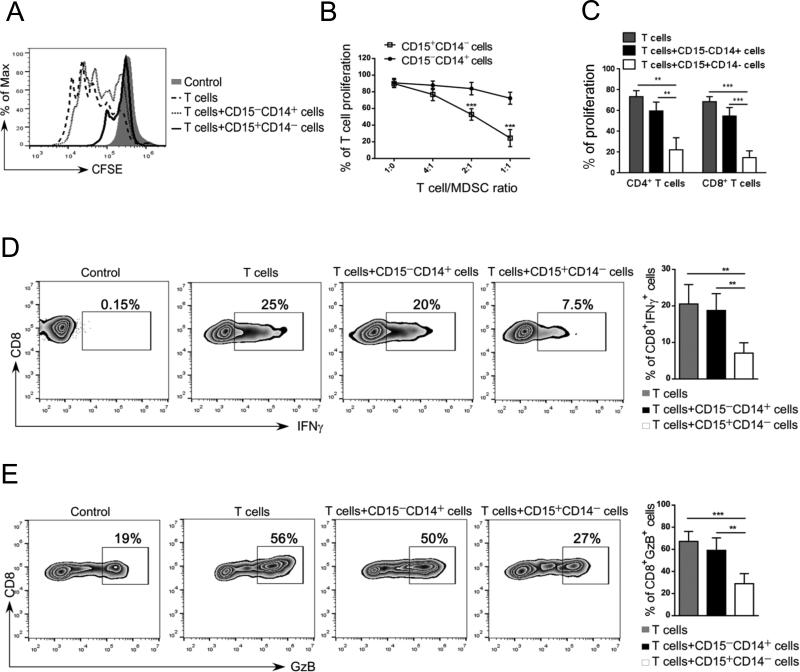
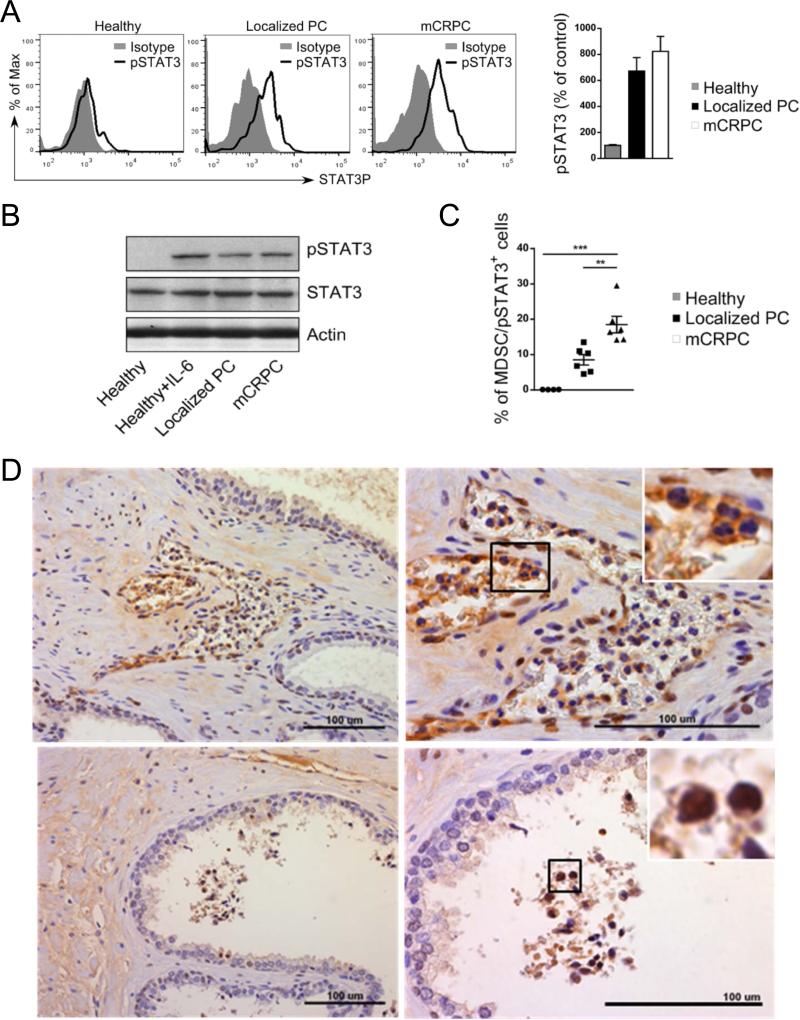
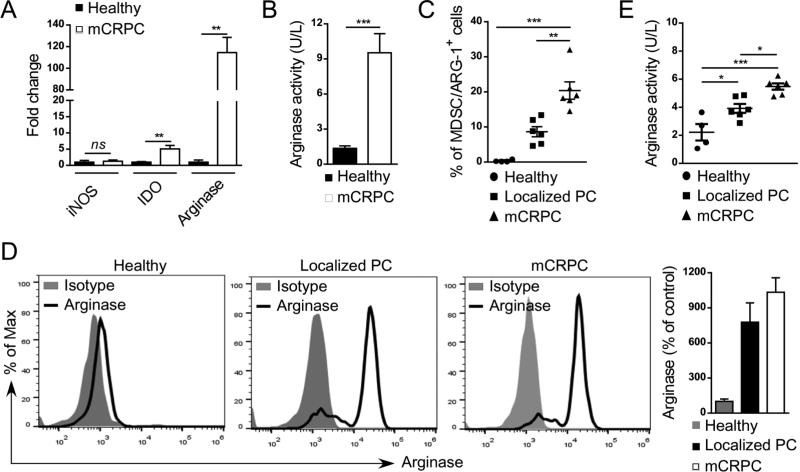
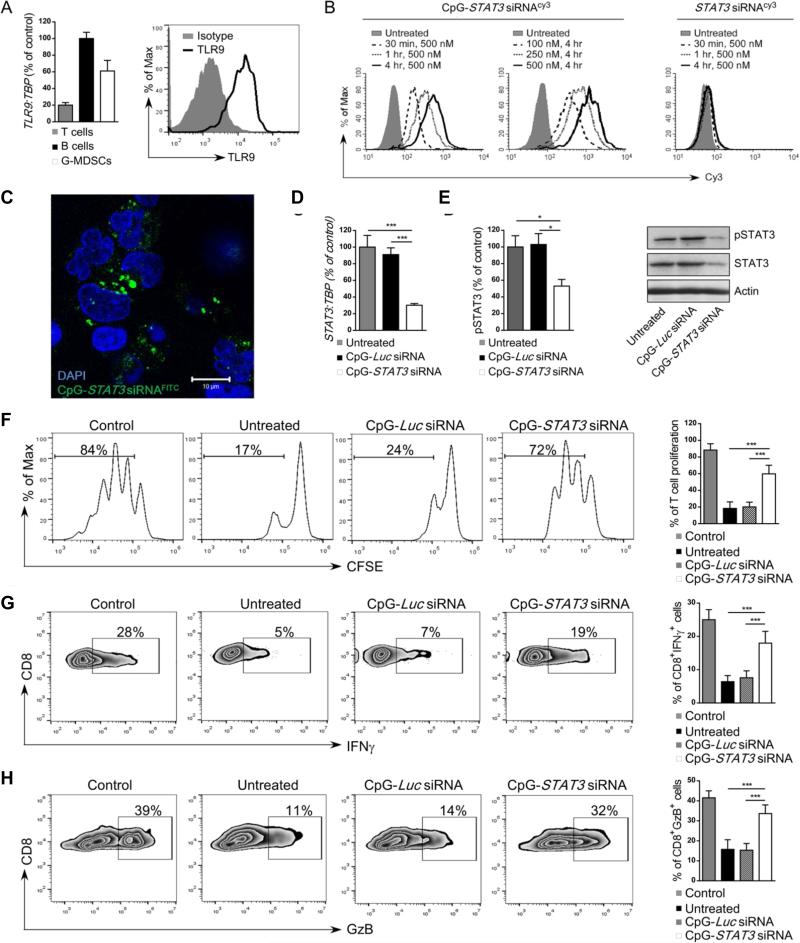
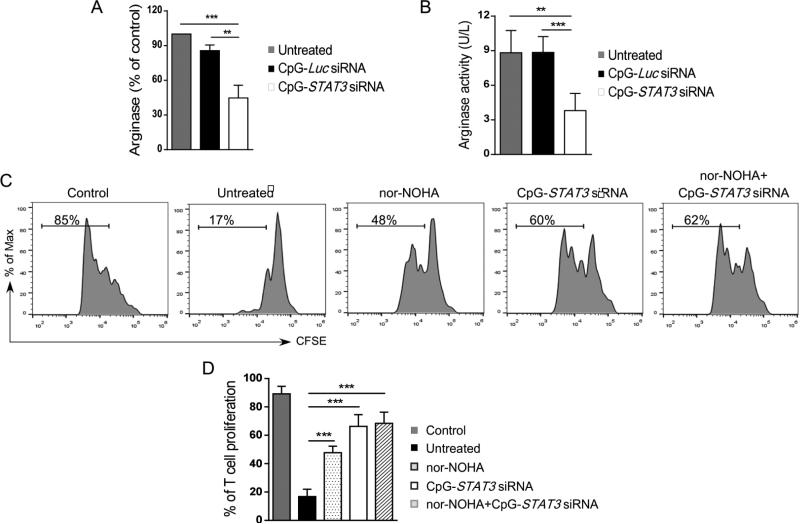
Results: Here, we identify a population of Lin(-)CD15(HI)CD33(LO) granulocytic MDSCs that accumulate in patients' circulation during prostate cancer progression from localized to metastatic disease. The prostate cancer-associated MDSCs potently inhibit autologous CD8(+) T cells' proliferation and production of IFNγ and granzyme-B. The circulating MDSCs have high levels of activated STAT3, which is a central immune checkpoint regulator. The granulocytic pSTAT3(+) cells are also detectable in patients' prostate tissues. We previously generated an original strategy to silence genes specifically in Toll-like Receptor-9 (TLR9) positive myeloid cells using CpG-siRNA conjugates. We demonstrate that human granulocytic MDSCs express TLR9 and rapidly internalize naked CpG-STAT3siRNA, thereby silencing STAT3 expression. STAT3 blocking abrogates immunosuppressive effects of patients-derived MDSCs on effector CD8(+) T cells. These effects depended on reduced expression and enzymatic activity of Arginase-1, a downstream STAT3 target gene and a potent T-cell inhibitor.
Conclusions: Overall, we demonstrate the accumulation of granulocytic MDSCs with prostate cancer progression and the feasibility of using TLR9-targeted STAT3siRNA delivery strategy to alleviate MDSC-mediated immunosuppression.
©2015 American Association for Cancer Research.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA: a cancer journal for clinicians. 2010;60:277–300. - PubMed
-
- de Bono JS, Oudard S, Ozguroglu M, Hansen S, Machiels JP, Kocak I, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet. 2010;376:1147–54. - PubMed
-
- Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ, Penson DF, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363:411–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
