

Implementation and Operational Research: Effects of Antenatal Care and HIV Treatment Integration on Elements of the PMTCT Cascade: Results From the SHAIP Cluster-Randomized Controlled Trial in Kenya
- PMID: 25967269
- PMCID: PMC4501892
- DOI: 10.1097/QAI.0000000000000678
Implementation and Operational Research: Effects of Antenatal Care and HIV Treatment Integration on Elements of the PMTCT Cascade: Results From the SHAIP Cluster-Randomized Controlled Trial in Kenya
Abstract
Background: Integrating antenatal care (ANC) and HIV care may improve uptake and retention in services along the prevention of mother-to-child transmission (PMTCT) cascade. This study aimed to determine whether integration of HIV services into ANC settings improves PMTCT service utilization outcomes.
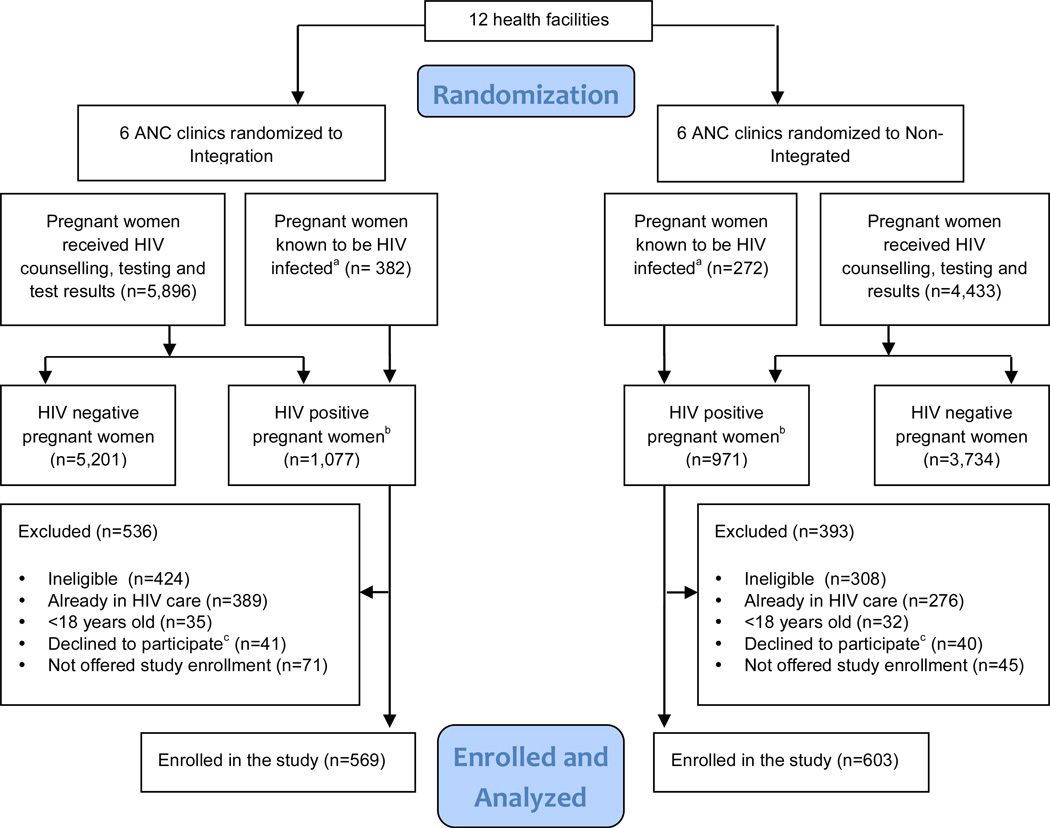
Methods: ANC clinics in rural Kenya were randomized to integrated (6 clinics, 569 women) or nonintegrated (6 clinics, 603 women) services. Intervention clinics provided all HIV services, including highly active antiretroviral therapy (HAART), whereas control clinics provided PMTCT services but referred women to HIV care clinics within the same facility. PMTCT utilization outcomes among HIV-infected women (maternal HIV care enrollment, HAART initiation, and 3-month infant HIV testing uptake) were compared using generalized estimating equations and Cox regression.
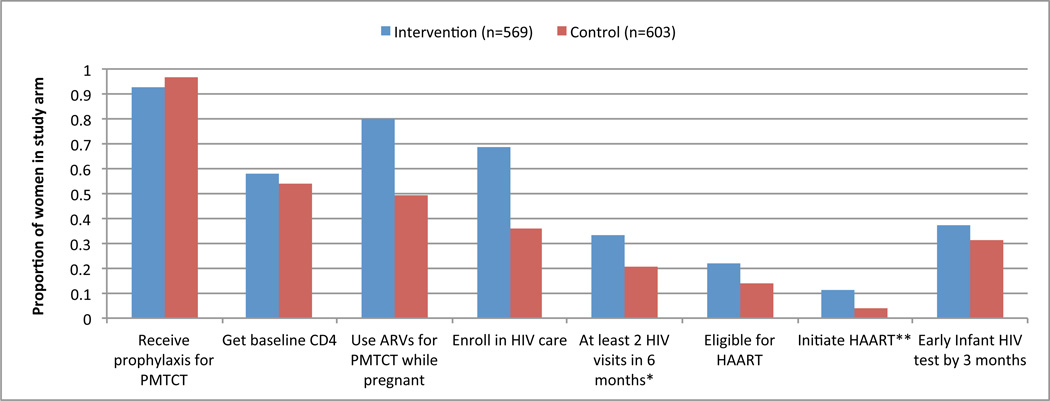
Results: HIV care enrollment was higher in intervention compared with control clinics [69% versus 36%; odds ratio = 3.94, 95% confidence interval (CI): 1.14 to 13.63]. Median time to enrollment was significantly shorter among intervention arm women (0 versus 8 days, hazard ratio = 2.20, 95% CI: 1.62 to 3.01). Eligible women in the intervention arm were more likely to initiate HAART (40% versus 17%; odds ratio = 3.22, 95% CI: 1.81 to 5.72). Infant testing was more common in the intervention arm (25% versus 18%), however, not statistically different. No significant differences were detected in postnatal service uptake or maternal retention.
Conclusions: Service integration increased maternal HIV care enrollment and HAART uptake. However, PMTCT utilization outcomes were still suboptimal, and postnatal service utilization remained poor in both study arms. Further improvements in the PMTCT cascade will require additional research and interventions.
Figures
References
-
- UNAIDS. Global report: UNAIDS report on the global AIDS epidemic. UNAIDS; 2010. p. 364.
-
- World Health Organisation. [Accessed December 4, 2012];PMTCT Strategic Vision 2010–2015: Preventing mother-to-child transmission of HIV to reach UNGASS and Millennium Development Goals. 2010 Available at: http://www.who.int/hiv/pub/mtct/strategic_vision.pdf.
-
- Townsend CL, Cortina-Borja M, Peckham CS, de Ruiter A, Lyall H, Tookey PA. Low rates of mother-to-child transmission of HIV following effective pregnancy interventions in the United Kingdom and Ireland, 2000–2006. AIDS. 2008 May 11;22(8):973–981. - PubMed
-
- Becquet R, Newell ML. Prevention of postnatal HIV infection: infant feeding and antiretroviral interventions. Current opinion in HIV and AIDS. 2007 Sep;2(5):361–366. - PubMed
-
- Médecins sans frontières. Responding to the failure of prevention of mother-to-child trans- mission (PMTCT) programmes: what needs to change? Expert roundtable 23. 2008 http://www.msfaccess.org/main/hiv-aids/pmtct-experts-roundtable/.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
