

The Gut as a Source of Inflammation in Chronic Kidney Disease
- PMID: 25967288
- PMCID: PMC4485546
- DOI: 10.1159/000381990
The Gut as a Source of Inflammation in Chronic Kidney Disease
Abstract
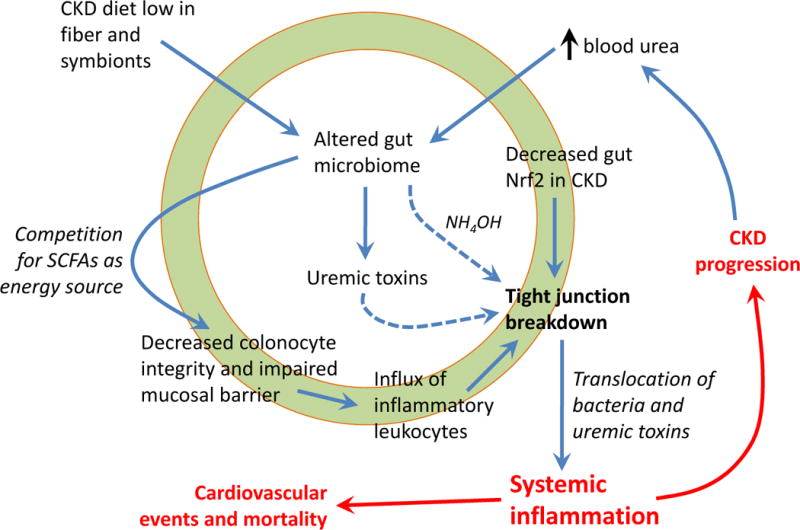
Chronic inflammation is a non-traditional risk factor for cardiovascular mortality in the chronic kidney disease (CKD) population. In recent years, the gastrointestinal tract has emerged as a major instigator of systemic inflammation in CKD. Postmortem studies previously discovered gut wall inflammation throughout the digestive tract in chronic dialysis patients. In CKD animals, colon wall inflammation is associated with breakdown of the epithelial tight junction barrier ('leaky gut') and translocation of bacterial DNA and endotoxin into the bloodstream. Gut bacterial DNA and endotoxin have also been detected in the serum from CKD and dialysis patients, whereby endotoxin levels increase with the CKD stage and correlate with the severity of systemic inflammation in the dialysis population. The CKD diet that is low in plant fiber and symbiotic organisms (in adherence with low potassium, low phosphorus intake) can alter the normal gut microbiome, leading to overgrowth of bacteria that produce uremic toxins such as cresyl and indoxyl molecules. The translocation of these toxins from the 'leaky gut' into the bloodstream further promotes systemic inflammation, adverse cardiovascular outcomes and CKD progression. Data are lacking on optimal fiber and yogurt consumption in CKD that would favor growth of a more symbiotic microbiome while avoiding potassium and phosphorus overload. Prebiotic and probiotic formulations have shown promise in small clinical trials, in terms of lowering serum levels of uremic toxins and improving quality of life. The evidence points to a strong relationship between intestinal inflammation and adverse outcomes in CKD, and more trials investigating gut-targeted therapeutics are needed.
© 2015 S. Karger AG, Basel.
Conflict of interest statement
KKZ has received honoraria from Abbott, Abbvie, Amgen, Genzyme/Sanofi, Otsuka, Shire, Vifor, and was the medical director of DaVita Harbor-UCLA/MFI in Long Beach, CA, during 2007–2012. Other authors have not declared any conflicts of interest.
Figures
Comment in
-
Genetic evidence supporting the causal role of gut microbiota in chronic kidney disease and chronic systemic inflammation in CKD: a bilateral two-sample Mendelian randomization study.Front Immunol. 2023 Nov 2;14:1287698. doi: 10.3389/fimmu.2023.1287698. eCollection 2023. Front Immunol. 2023. PMID: 38022507 Free PMC article.
References
-
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382(9889):339–352. - PubMed
-
- Kalantar-Zadeh K, Ikizler TA, Block G, Avram MM, Kopple JD. Malnutrition-inflammation complex syndrome in dialysis patients: causes and consequences. Am J Kidney Dis. 2003;42(5):864–881. - PubMed
-
- Kendrick J, Chonchol MB. Nontraditional risk factors for cardiovascular disease in patients with chronic kidney disease. Nat Clin Pract Nephrol. 2008;4(12):672–681. - PubMed
-
- Lau WL, Ix JH. Clinical detection, risk factors, and cardiovascular consequences of medial arterial calcification: a pattern of vascular injury associated with aberrant mineral metabolism. Semin Nephrol. 2013;33(2):93–105. - PubMed
-
- Carrero JJ, Stenvinkel P. Persistent inflammation as a catalyst for other risk factors in chronic kidney disease: a hypothesis proposal. Clin J Am Soc Nephrol. 2009;4(Suppl 1):S49–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
