

Serum uric acid and the incidence of CKD and hypertension
- PMID: 25967597
- PMCID: PMC4679779
- DOI: 10.1007/s10157-015-1120-4
Serum uric acid and the incidence of CKD and hypertension
Abstract
Background: Uric acid (UA) levels correlate positively with the prevalence of chronic kidney disease (CKD) and/or hypertension. We tested the hypothesis that UA may also have a link to a new incidence of CKD and hypertension.
Methods: Study design is a cohort study and the predictor is UA levels. Of the 15,470 screened cases, 8223 participants without CKD were eligible for the analysis of the incidence of CKD. Among these CKD candidates, 7569 participants were eligible for the analysis of the new development of hypertension. The observation period was 4 years.
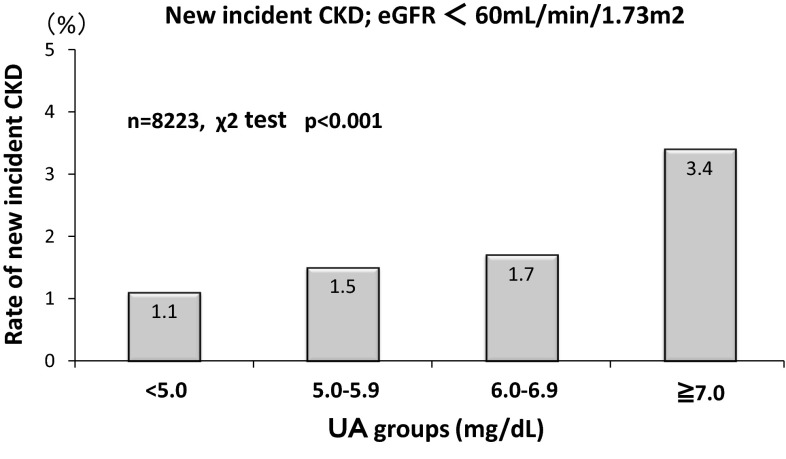
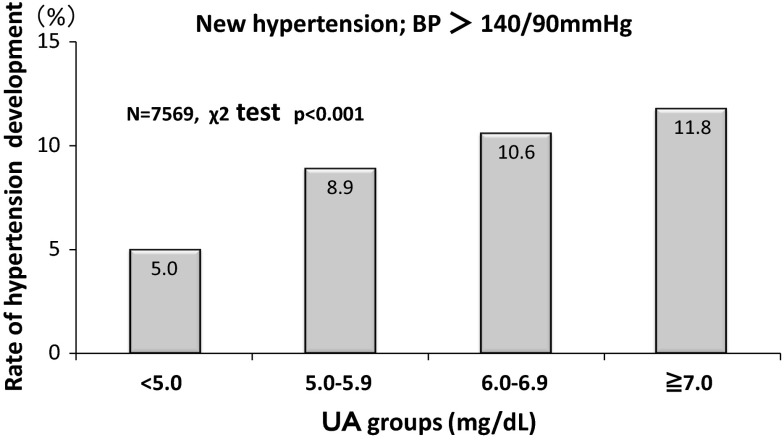
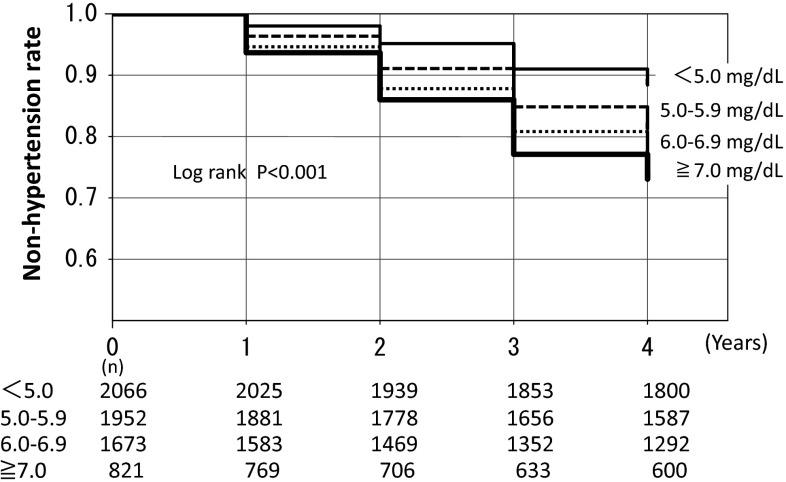
Results: Relationship of UA with new cases of CKD. Higher UA levels had a closer association with the new development of CKD; 1.1 % (UA < 5 mg/dL), 1.5 % (5.0-5.9 mg/dL), 1.7 % (6.0-6.9 mg/dL), and 3.4 % (≧7 mg/dL), respectively (p < 0.001 by the Chi-square test). Cox proportional hazard analysis showed that the estimates of the CKD development were eGFR [Hazard Ratio (HR) 0.816, 95 % confidence intervals (CI) 0.791-0.840] and male gender (HR 0.562, 95 % CI 0.322-0.982). UA levels and new development of hypertension. Higher UA levels had a closer association with the new development of hypertension; 5.0 % (UA < 5 mg/dL), 8.9 % (5.0-5.9 mg/dL), 10.6 % (6.0-6.9 mg/dL), and 11.8 % (≧7 mg/dL), respectively (p < 0.001 by the Chi-square test). Cox proportional hazard analysis showed that the estimates of the hypertension development were BMI (HR 1.190, 95 % CI 1.155-1.226), age (HR 1.021, 95 % CI 1.010-1.032), HDL-cholesterol (HR 1.013, 95 % CI 1.007-1.019), male gender (HR 1.791, 95 % CI 1.338-2.395), UA level (HR 1.112, 95 % CI 1.024-1.207), and eGFR (HR 1008, 95 % CI 1.002-1.013). Furthermore, the logistic analysis showed that the odds ratio (OR) to estimate hypertension in the high UA group (UA ≧ 7 mg/dL; OR 1.33, 95 % CI 1.01-1.80) was greater than that in the low UA group (UA < 5 mg/dL). Kaplan-Meier analysis also confirmed the finding that the higher the UA levels the greater the hypertension development (p < 0.001 by the Log-rank test and Cox proportional hazard analysis).
Conclusion: High UA levels are associated with the new development of hypertension, but not with the incidence of CKD.
Keywords: CKD; Estimated glomerular filtration rate; Hypertension; Uric acid.
Figures
Similar articles
-
Uric acid and incident chronic kidney disease in a large health check-up population in Taiwan.Nephrology (Carlton). 2011 Nov;16(8):767-76. doi: 10.1111/j.1440-1797.2011.01513.x. Nephrology (Carlton). 2011. PMID: 21854506
-
Uric acid and incident chronic kidney disease in dyslipidemic individuals.Curr Med Res Opin. 2018 Jul;34(7):1193-1199. doi: 10.1080/03007995.2017.1372157. Epub 2017 Sep 21. Curr Med Res Opin. 2018. PMID: 28836857
-
Association of uric acid and left ventricular mass index with renal outcomes in chronic kidney disease.Am J Hypertens. 2013 Feb;26(2):243-9. doi: 10.1093/ajh/hps020. Epub 2012 Dec 28. Am J Hypertens. 2013. PMID: 23382409
-
Serum Uric Acid and Progression of Kidney Disease: A Longitudinal Analysis and Mini-Review.PLoS One. 2017 Jan 20;12(1):e0170393. doi: 10.1371/journal.pone.0170393. eCollection 2017. PLoS One. 2017. PMID: 28107415 Free PMC article. Review.
-
A systematic review and meta-analysis of the association between uric acid levels and chronic kidney disease.Sci Rep. 2022 Apr 15;12(1):6251. doi: 10.1038/s41598-022-10118-x. Sci Rep. 2022. PMID: 35428828 Free PMC article.
Cited by
-
Dotinurad: a novel selective urate reabsorption inhibitor as a future therapeutic option for hyperuricemia.Clin Exp Nephrol. 2020 Mar;24(Suppl 1):1-5. doi: 10.1007/s10157-019-01811-9. Epub 2019 Nov 21. Clin Exp Nephrol. 2020. PMID: 31754883 Free PMC article. Review.
-
Targeting Uric Acid and the Inhibition of Progression to End-Stage Renal Disease--A Propensity Score Analysis.PLoS One. 2015 Dec 23;10(12):e0145506. doi: 10.1371/journal.pone.0145506. eCollection 2015. PLoS One. 2015. PMID: 26700005 Free PMC article.
-
Pathophysiology of hyperuricemia and its clinical significance - a narrative review.Reumatologia. 2020;58(5):312-323. doi: 10.5114/reum.2020.100140. Epub 2020 Oct 29. Reumatologia. 2020. PMID: 33227090 Free PMC article. Review.
-
Associations between serum uric acid levels and the incidence of nonfatal stroke: a nationwide community-based cohort study.Clin Exp Nephrol. 2017 Jun;21(3):497-503. doi: 10.1007/s10157-016-1311-7. Epub 2016 Jul 12. Clin Exp Nephrol. 2017. PMID: 27405620
-
Effect of hyperuricemia and treatment for hyperuricemia in Japanese hemodialysis patients: A cohort study.PLoS One. 2019 Jun 6;14(6):e0217859. doi: 10.1371/journal.pone.0217859. eCollection 2019. PLoS One. 2019. PMID: 31170241 Free PMC article.
References
-
- Jossa F, Farinaro E, Panico S, Krogh V, Celentano E, Galasso R, Mancini M, Trevisan M. Serum uric acid and hypertension: the Olivetti Heart Study. J Hum Hypertens. 1994;8:677–681. - PubMed
-
- Mellen PB, Bleyer AJ, Erlinger TP, Evans GW, Nieto FJ, Wagenknecht LE, Wofford MR, Herrington DM. Serum uric acid predicts incident hypertension in a biethnic cohort: the atherosclerosis risk in communities study. Hypertension. 2006;48(6):1037–1042. doi: 10.1161/01.HYP.0000249768.26560.66. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
