

Development of a novel IGRA assay to test T cell responsiveness to HBV antigens in whole blood of chronic Hepatitis B patients
- PMID: 25968473
- PMCID: PMC4465460
- DOI: 10.1186/s12967-015-0513-1
Development of a novel IGRA assay to test T cell responsiveness to HBV antigens in whole blood of chronic Hepatitis B patients
Abstract
Background: Interferon gamma release assays (IGRA) have been developed to support easy and fast diagnosis of diseases like tuberculosis, and CMV in transplant patients. IGRAs focus on cellular immunity especially memory T cells and thus also allow rapid screening prior to complex flow cytometric testing. Here, we describe a novel, sensitive whole blood based cytokine release assay capable of assessing T cell responsiveness to HBV antigens in Hepatitis B patients and assessing hepatitis B vaccination status in healthy individuals.
Methods: Seventy two chronic Hepatitis B patients (CHB), 8 acute hepatitis B patients (AHB) and 80 healthy controls (HC) were tested by ELISA for IFNγ- and IL2-secretion in whole blood after challenge with synthetic peptide libraries of hepatitis B core antigen (HBcAg) or hepatitis B surface antigen (HBsAg).
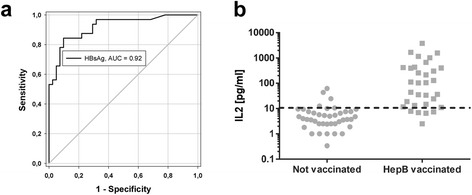
Results: The developed IGRA test reliably differentiated between Hepatitis B patients, vaccinees and unvaccinated healthy controls. Treatment naïve and treated CHB patients showed a weaker IFNγ response to HBcAg (16 ± 5 and 35 ± 28 pg/ml, respectively) compared to the AHB group (82 ± 39 pg/ml), whereas HC remained unresponsive (6 ± 1 pg/ml). IL2 levels after HBcAg challenge were also higher in the AHB group compared to naive and treated CHB as well as HC (47 ± 21 vs. 12 ± 3, 15 ± 10 and 12 ± 9 pg/ml, respectively). HBsAg stimulation led to increased IFNγ and IL2 levels in the AHB group (33 ± 12 and 22 ± 12 pg/ml) and even higher levels in HC due to a high hepatitis B vaccination rate (41 ± 10 and 167 ± 58 pg/ml). Naive and treated CHB patients developed no or only weaker IFNγ or IL2 responses to HBsAg (5 ± 2 and 12 ± 7 pg/ml, for naive CHB, 12 ± 10 and 18 ± 15 pg/ml, for treated CHB). For HC, IL2 release after HBsAg stimulation depicted hepatitis B vaccination status with a diagnostic sensitivity and specificity of 85 % and 90 %.
Conclusion: Our novel whole blood based cytokine release assay constitutes an easy and robust tool for screening HBV specific cellular immunity as alternative to flow cytometry or ELISPOT assays.
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
