

Does Coordinated, Multidisciplinary Treatment Limit Medical Disability and Attrition Related to Spine Conditions in the US Navy?
- PMID: 25968894
- PMCID: PMC4523524
- DOI: 10.1007/s11999-015-4328-4
Does Coordinated, Multidisciplinary Treatment Limit Medical Disability and Attrition Related to Spine Conditions in the US Navy?
Abstract
Background: Musculoskeletal conditions account for the largest proportion of cases resulting in early separation from the US Navy. This study evaluates the impact of the Spine Team, a multidisciplinary care group that included physicians, physical therapists, and a clinical psychologist, for the treatment of active-duty service members with work-disabling, nonspecific low back pain at the Naval Medical Center, Portsmouth, VA, USA. We compared the impact of the introduction of the Spine Team in limiting disability and attrition from work-disabling spine conditions with the experience of the Naval Medical Center, San Diego, CA, USA, where there is no comparable spine team.
Questions/purposes: Is a multidisciplinary spine team effective in limiting disability and attrition related to work-disabling spine conditions as compared with the current standard of care for US military active-duty service members?
Methods: This is a retrospective, pre-/post-study with a separate, concurrent control group using administratively collected data from two large military medical centers during the period 2007 to 2009. In this study, disability is expressed as the proportion of active-duty service members seeking treatment for a work-disabling spine condition that results in the assignment of a first-career limited-duty status. Attrition is expressed as the proportion of individuals assigned a first-career limited-duty status for a work-disabling spine condition who were referred to a Physical Evaluation Board. We analyzed 667 individuals assigned a first-career limited-duty for a work-disabling spine condition between 2007 and 2009 who received care at the Naval Medical Center Portsmouth or Naval Medical Center San Diego.
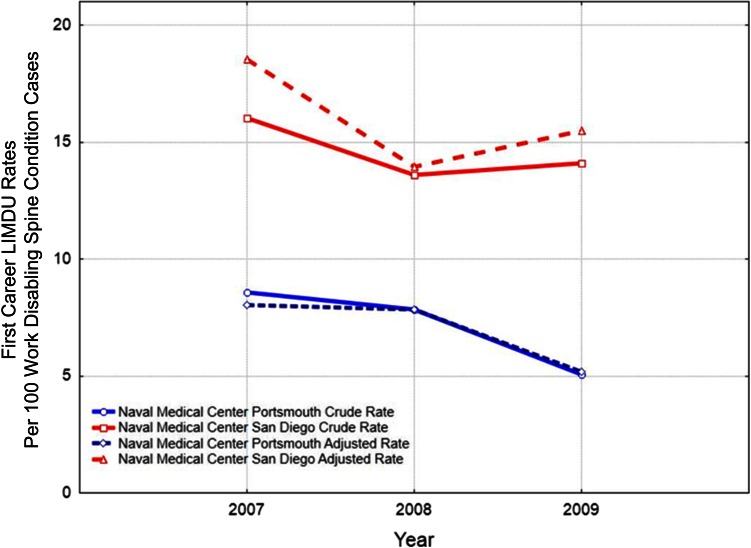
Results: Rates of first-career limited-duty assignments for spine conditions decreased from 2007 to 2009 at both sites, but limited-duty rates decreased to a greater extent at the intervention site (Naval Medical Center Portsmouth; from 8.5 per 100 spine cases in 2007 to 5.1 per 100 cases in 2009, p < 0.001) as compared with the control site (Naval Medical Center San Diego; 16.0 per 100 spine cases in 2007 and 14.1 per 100 cases in 2009, p = 0.38) after the Spine Team was implemented in 2008. The risk of disability was lower at Naval Medical Center Portsmouth as compared with Naval Medical Center San Diego for each of the 3 years studied (in 2007, the relative risk was 0.53 [95% confidence limit {CL}, 0.42-0.68; p < 0.001]) indicating a protective effect of Naval Medical Center Portsmouth in limiting disability (in 2008, it was 0.58 [95% CL, 0.45-0.73; p < 0.001] and in 2009 0.34 [95% CL, 0.27-0.47; p < 0.001]); the relative risk improved in 2009 after the introduction of the Spine Team at Naval Medical Center Portsmouth. There were no differences observed in rates of attrition from the period before the introduction of the Spine Team to after at Naval Medical Center Portsmouth, and no overall differences could be statistically detected between the two sites.
Conclusions: This study provides suggestive evidence that a multi-disciplinary Spine Team may be effective in limiting disability. No conclusion can be drawn about the Spine Team's effectiveness in limiting attrition. Additional study is warranted to examine the effect of the timing of the introduction of multidisciplinary care for work-disabling spine conditions.
Level of evidence: Level III, therapeutic study.
Figures
References
-
- Accident Compensation Corporation. New Zealand Acute Low Back Pain Guide, Incorporating the Guide to Assessing Psychosocial Yellow Flags in Acute Low Back Pain. 2004. Available at: http://www.acc.co.nz/PRD_EXT_CSMP/groups/external_communications/documen.... Accessed April 20, 2015.
-
- Anema JR, Steenstra IA, Bongers PM, de Vet HC, Knol DL, Loisel P, van Mechelen W. Multidisciplinary rehabilitation for subacute low back pain: graded activity or workplace intervention or both? A randomized controlled trial. Spine. 2007;32:291–298; discussion 299–300. - PubMed
-
- Armitage P. Tests for linear trends in proportions and frequencies. Biometrics. 1955;11:375–386. doi: 10.2307/3001775. - DOI
-
- Berkowitz SM, Feuerstein M, Lopez MS, Peck CA., Jr Occupational back disability in US Army personnel. Mil Med. 1999;164:412–418. - PubMed
-
- Bohnker BK, Telfair T, McGinnis JA, Malakooti MA, Sack DM. Analysis of Navy Physical Evaluation Board diagnoses (1998-2000) Mil Med. 2003;168:482–485. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
